Definition/Introduction
Primitive reflexes are innate, automatic motor patterns and reactions emerging during fetal life until after birth crucial for an infant's survival. These reflexes are being integrated and replaced gradually in term infants into higher-level righting, support, and protective postural reactions. This dynamic transition is part of the neuropsychomotor organization and development, physiological maturation, fine-tuning of the nervous system, which includes motor centers in the brainstem to the cerebral cortex - occurring in response to increasing environmental influences and demands. The involved reflex integration allows a change in the quality of movements, from clumsy to more natural, spontaneous, and efficient sensory processing, internal postural control, and acquired, goal-directed, precise, and well-coordinated voluntary motor skills and movements against gravity, which in effect, affect learning and behavior of a child in his later stages of life.[1][2][3][4][5][4][6][7][8]
Some studies also mentioned primitive reflexes' unconscious influence and their use in response to both stressful and nonstressful conditions in healthy older children and neurologically intact adults. This "reflex recruitment" allows the production of the desired movement with greater efficiency despite motor stress and is demonstrated in athletic postures, including asymmetric tonic neck reflex (ATNR) in the volley in tennis and the lunge position in fencing to increase upper-arm strength during resisted movement. Additionally, primitive reflexes could have synergistic and antagonistic effects, such as the case of interaction between the tonic labyrinth and neck proprioceptors. The antagonistic actions of the labyrinth reflex for the head tilt or rotation are opposed by the neck reflexes causing upright trunk posture and stabilizing action to extremities (no net movement) acting as a single system.[1][3][4][5][6][7][8][9]
ATNR is a primitive reflex that appears 18 weeks in utero, most prominent between 1 and 4 months of age, and disappears by 3 to 9 months after birth. This reflex is produced by rotating the head to one side, causing the ipsilateral extension of the extremities towards which the face is turned and contralateral flexion of extremities. This reflex is essential for postural tone and stability, gross and fine movements, eye tracking, and midline crossing crucial for reading, telling the time, left-right discrimination, etc. On the other hand, symmetrical tonic neck reflex (STNR) appears 6 to 9 months after birth until 9 to 11 months of age. This reflex is elicited by moving the head up and down passively with subsequent upper extremity flexion and lower extremity extension with neck flexion while neck extension produces upper extremity extension and lower extremity flexion. This reflex is significant for posture, eye-hand coordination, and focus required in activities like sitting, swimming, playing with a ball, etc. This postural tone is influenced by cortical and subcortical structures, including somatic descending brain stem pathways, descending fiber tracts of monoaminergic systems pathways, and limbic system.[1][2][10][6][11]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Development of psychomotor, social, educational, and communication skills is inhibited with persistence or re-emergence of primitive reflexes demonstrated in patients with brain damages, such as cerebral palsy or stroke. Several studies discussed strong predictive properties of retained spontaneous (not evoked) ATNR in infants with high perinatal risk factors for cerebral palsy and developmental disorders with increasing age. More severe primitive reflex patterns resulted in more developmental retardation. However, the criteria for the presence and absence of primitive reflexes and their corresponding predictive abnormality are age-dependent, as a whole.[1][2][7]
Clinical Significance
Neurological insults, such as cerebral palsy and post-cerebrovascular accident (CVA), damage the nervous system's sensorimotor integration, manifested with the reemergence and disinhibition of primitive stereotyped reflexes. In one study, the presence and the seemingly exaggerated response of ATNR due to the relative dominance of the primitive reflexes with loss of higher-level reactions in spastic hemiplegic patients were investigated and compared with neurologically intact adults. ATNR is elicited through several voluntary resisted active rotation of the head. These primitive reflexes serve as an indicator of the reversal of the central nervous system's motor control. Also, the antagonistic actions between tonic labyrinthine reflex and ATNR still manifest in these patients.[6][8]
The persistence of primitive reflexes, such as tonic neck reflexes and spinal Galant reflex, is also studied in the development of muscle tone asymmetry, faulty posture, and spinal deformities. This process occurs by measuring the angle of trunk rotation (ATR) to evaluate scoliosis and prevent its progression. This angle is an early objective assessment of trunk rotation, which appears to be influenced by ATNR, in the growing spine of children.[7]
Nursing, Allied Health, and Interprofessional Team Interventions
Rehabilitation goals may aim in balancing the use of primitive reflexes such as ATNR to increase posture, balance, hand function, and movement of patients to achieve a task while reintegrating these reflexes into a higher level of postural control. This process should be part of the neuromuscular re-education programs for stroke patients and is also essential during primitive reflex integration therapy, which includes repeating mimic movement patterns from the first year of life for children with low psychomotor skills and skeletal deformities with correction at the basic neurological level. By introducing carefully the factors producing motor stress, such as gravity, the complexity of the movement required, and requirements of the activity or skill, into the treatment program, the appearance of primitive reflexes gives a hint on the level of difficulty and demand of the tasks. Once the patient is observed to rely on primitive reflex as his maladaptive response, the task should be modified appropriately to allow normal responses and functions. The reflexes then serve as a feedback mechanism to analyze the patient's movement and not as a mere symptom to be corrected.[1][6][7]
Nursing, Allied Health, and Interprofessional Team Monitoring
One study discussed the recurring sustained posturing reflecting the strength of reflex activity (not only the presence or absence of ATNR) in preterm infants predicted subsequent abnormal development. This research emphasized the value of comprehensive neurological assessments being beneficial, especially if done longitudinally across the development of high-risk preterm and term infants, even while in the intensive and/or special care nursery, in predicting their susceptibility to developmental disorders. Starting therapeutic goals early, such as in infant handling and positioning and supportive parental instructions, are crucial for holistic management and rehabilitation to these patients. Another study mentioned an ATNR rating scale that can be used as a clinical quantitative tool to assess patients with suspected or known sensory integration deficits, maturational, learning, or behavioral delays. Several works of literature also proposed the conduction of routine neurological examinations of the degree of reflexes integration in children. The results should correlate to factors such as trunk rotation, psychomotor skills, and neurodevelopment for early and more effective management. All these assessments may prevent the progression of psychomotor, social, and educational delays on a personal level and lessen the high cost of healthcare at the societal level.[1][2][7][8][9][11][12]
Media
(Click Image to Enlarge)
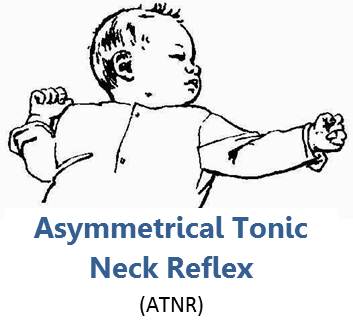
Asymmetrical Tonic Neck Reflex Contributed by Creative Commons, Ashley Arbuckle, (CC BY 2.0) https://creativecommons.org/licenses/by/2.0/deed.en
(Click Image to Enlarge)
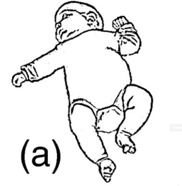
Asymmetrical tonic neck reflex elicited by rotating the head to one side causing ipsilateral extension of the extremities towards which the face is turned and contralateral flexion of extremities. Contributed from Hamer EG, Hadders-Algra M. Prognostic significance of neurological signs in high-risk infants - a systematic review. Dev Med Child Neurol. 2016;58 Suppl 4:53‐60. doi:10.1111/dmcn.13051 Free Access PMID: 27027608
References
Gieysztor EZ, Choińska AM, Paprocka-Borowicz M. Persistence of primitive reflexes and associated motor problems in healthy preschool children. Archives of medical science : AMS. 2018 Jan:14(1):167-173. doi: 10.5114/aoms.2016.60503. Epub 2016 Jun 13 [PubMed PMID: 29379547]
Hamer EG, Hadders-Algra M. Prognostic significance of neurological signs in high-risk infants - a systematic review. Developmental medicine and child neurology. 2016 Mar:58 Suppl 4():53-60. doi: 10.1111/dmcn.13051. Epub [PubMed PMID: 27027608]
Level 1 (high-level) evidenceLindsay KW, Roberts TD, Rosenberg JR. Asymmetric tonic labyrinth reflexes and their interaction with neck reflexes in the decerebrate cat. The Journal of physiology. 1976 Oct:261(3):583-601 [PubMed PMID: 978589]
Level 3 (low-level) evidenceDutia MB, Lindsay KW, Rosenberg JR. The effect of cerebellectomy on the tonic labyrinth and neck reflexes in the decerebrate cat. The Journal of physiology. 1981 Mar:312():115-23 [PubMed PMID: 7264988]
Level 3 (low-level) evidenceKuiper MJ, Brandsma R, Lunsing RJ, Eggink H, Ter Horst HJ, Bos AF, Sival DA. The neurological phenotype of developmental motor patterns during early childhood. Brain and behavior. 2019 Jan:9(1):e01153. doi: 10.1002/brb3.1153. Epub 2018 Nov 28 [PubMed PMID: 30485703]
Warren ML. A comparative study on the presence of the asymmetrical tonic neck reflex in adult hemiplegia. The American journal of occupational therapy : official publication of the American Occupational Therapy Association. 1984 Jun:38(6):386-92 [PubMed PMID: 6742088]
Level 1 (high-level) evidenceGieysztor EZ, Sadowska L, Choińska AM, Paprocka-Borowicz M. Trunk rotation due to persistence of primitive reflexes in early school-age children. Advances in clinical and experimental medicine : official organ Wroclaw Medical University. 2018 Mar:27(3):363-366. doi: 10.17219/acem/67458. Epub [PubMed PMID: 29558021]
Level 3 (low-level) evidenceChinello A, Di Gangi V, Valenza E. Persistent primary reflexes affect motor acts: Potential implications for autism spectrum disorder. Research in developmental disabilities. 2018 Dec:83():287-295. doi: 10.1016/j.ridd.2016.07.010. Epub 2016 Aug 29 [PubMed PMID: 27595468]
Parmenter CL. An asymmetrical tonic neck reflex rating scale. The American journal of occupational therapy : official publication of the American Occupational Therapy Association. 1983 Jul:37(7):462-5 [PubMed PMID: 6614125]
Gurfinkel V, Cacciatore TW, Cordo P, Horak F, Nutt J, Skoss R. Postural muscle tone in the body axis of healthy humans. Journal of neurophysiology. 2006 Nov:96(5):2678-87 [PubMed PMID: 16837660]
Zemke R. Application of an ATNR rating scale to normal preschool children. The American journal of occupational therapy : official publication of the American Occupational Therapy Association. 1985 Mar:39(3):178-80 [PubMed PMID: 2581451]
Lacey JL, Henderson-Smart D, Edwards D, Storey B. Neurological assessment of the preterm infant in the special care nursery and the diagnostic significance of the asymmetrical tonic neck reflex. The Australian journal of physiotherapy. 1987:33(3):135-42. doi: 10.1016/S0004-9514(14)60590-0. Epub [PubMed PMID: 25025702]