Introduction
Ultrasound use in establishing intravenous access has been extensively documented for over 20 years and is now routinely performed in many settings for nonemergent central line placements and difficult peripheral intravenous access. The literature has proven this procedure's safety and high success rate, thus its widespread integration in emergency departments (see Video. Forearm Anatomy Review and Ultrasound Probing). While not as commonly undertaken, ultrasound can also be utilized for arterial access and cannulation. Once mastered, the procedure is simple, effective, and safe—with little to no increased risk or contraindications. Limitations to using ultrasound for establishing intravenous access include the availability of ultrasound machines and the required training. Any time a procedure is contemplated, the alternatives should be considered as well. The primary alternatives to ultrasound-guided intravenous access are anatomic landmark-guided placement (traditional) and using the intraosseous, intramuscular, and oral routes, bypassing intravenous access. Other alternative adjuncts to aid intravenous access include devices made for transillumination.[1][2][3]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
One must differentiate between an artery and a vein before cannulation. Knowledge of anatomy and their different characteristics on ultrasound can help distinguish these vessels. Veins are easily compressible when pressure is applied using the ultrasound probe, whereas arteries generally do not collapse. Pressure applied to arteries also creates a pulsatile movement (see Video. Ultrasound Assessment for Intravenous Placement). Arteries also have slightly thicker and more hyperechoic walls than veins.
With hypotension or vessel calcifications, these differences may not be as noticeable. In these cases, the color flow mode or Doppler mode may assist in differentiating between the artery and vein (see Image. Color Doppler Ultrasound of Artery versus Vein). When using color flow mode, the different colors do not inherently represent arteries or veins but the direction of blood flow toward or away from the probe. The operator should thus be careful when angling the probe and interpreting the color based on the probe’s angulation. When using Doppler flow, arteries generally show much greater velocity waveform variation than veins.
Once the proper vessel is identified, the path of the vessel must be followed to identify any branching or tortuosity that may complicate the cannulation. Viewing in longitudinal or transverse planes can help with this task.[4][5][6] Surrounding structures like nerves and their proximity to the vessel should be assessed to know the margin of error for complications in case of catheter misplacement. Ultrasound scanning of vessels helps identify the safest and most successful cannulation site.
Indications
Ultrasound guidance may be used for any patient, though it is typically prioritized for individuals with difficult intravenous access, either known previously or suspected. Patients undergoing high-risk procedures, such as internal jugular venous access, or who have already had failed attempts at establishing intravenous access may also benefit from ultrasound guidance.[7][8][9] Patients with suspected difficult access may include those with a history of intravenous drug use or hemodialysis or who presently have hypotension, dehydration, coagulopathy, chemoradiation, obesity, and edema. Very young children are also at risk of difficult access. Ultrasound intravenous access may be required for contrast enhancement during imaging, delivery of medications, fluids, or blood, and diagnostic procedures. Ultrasound intravenous access may also be used for arterial access to obtain diagnostic blood samples and for placing lines for monitoring purposes.
Contraindications
Ultrasound-guided intravenous access has no absolute contraindications. However, inadequate training or experience may lead to incorrect identification of structures and subsequent complications. A relative contraindication is when previous attempts have failed or when time is critical. In such cases, intraosseous access or landmark identification may provide quicker access. Other relative contraindications include conditions that may benefit more from traditional intravenous access than the ultrasound-guided approach, including insertion site burn, infection, injury, mastectomy, deep vein thrombosis, and arteriovenous fistula. Clinical judgment must be used in these instances. As the procedure's use becomes more widespread, the lack of training or experience will become less common. Many medical schools have begun implementing ultrasound curricula, and residency programs with ultrasound fellowship-trained faculty are increasing.
Equipment
Besides the supplies necessary for vascular access, an ultrasound machine with a high-frequency capable probe is all that is necessary. Full sterile precautions are also required if the procedure is for central access. Equipment designs vary. Thus, clinicians should be familiar with the specific ultrasound machines of their home institutions. The ultrasound probe indicator is a bump or marking on the side of the probe that correlates with a marker on one side of the screen (generally the left) for location identification. The probe indicator should align with the screen marker to ensure the probe's movements match those on the screen.
The correct orientation is usually achieved by positioning the probe marker toward the patient's right side. The machine should also have vertical markers on the screen to indicate the depth of the structures seen, which can be adjusted based on the target vessel's depth. Long angiocatheters should be used for accessing deep veins.
Personnel
Most trained personnel do not require the presence of another clinician for the procedure. The individual responsible for ultrasound-guided intravenous access may vary based on the institution and the vessel to be accessed and may include technicians, nurses, advanced practice clinicians, and physicians.
Preparation
As with most procedures, preparation is crucial for obtaining ultrasound-guided intravenous access. The steps vary depending on whether peripheral or central vein placement is being attempted. Universal precautions should always be observed to decrease the risk of infection transmission. The general conduct of the procedure should be discussed with the patient to alleviate anxiety. Consent can be obtained if time permits.
The following materials should be available at the bedside:
- Intravenous line starting kit (tourniquet band, appropriate length intravenous catheter, and antiseptic solution)
- Intravenous flushes
- Saline lock
- Ultrasound with a high-frequency linear probe
- Sterile gel
- Sterile probe cover
For peripheral intravenous access, a thin adhesive dressing such as Tegaderm may be used to cover the ultrasound probe. Common sites when performing ultrasound-guided intravenous access include the superficial veins of the hand and forearm, antecubital fossa, external jugular vein, and the upper arm's deeper basilic, brachial, or cephalic veins. The most accessible approach when identifying the deep upper arm veins is usually from the arm's medial side. For central intravenous access, sites include the femoral, subclavian, and internal jugular veins.
Technique or Treatment
The different approaches to ultrasound-guided intravenous access include the static, real-time, longitudinal, and transverse methods. In the static approach, the vessel is identified, and a skin marking is made at the site of the proper needle entry point. The course of the vein and anticipated point of vessel contact may also be marked. The probe is then put down, the site is sterilized, and intravenous access is attempted. This approach alleviates the need for a sterile probe covering and maintaining the ultrasound probe on the patient during the procedure. The success rate is much lower for this method when compared to the real-time approach.
In the real-time method, a sterile probe cover is placed on the ultrasound probe, and the ultrasound is used to visually guide the needle dynamically during the procedure. The success rate for this method is higher, allowing for fewer attempts and higher patient satisfaction. With the longitudinal approach, the vessel appears as a long cylindrical structure. This approach enables visualization of the entire needle while attempting to cannulate the vessel. The ultrasound probe, for the most part, remains still while the needle is guided into place. In this view, the ultrasound beam, needle, and vessel must align in the same plane, complicating lateral needle movements and making it challenging to determine the needle's lateral position relative to the vessel. This approach is more difficult for curved or tortuous vessels.
In the transverse or short-axis approach, the vessel appears circular. Needle placement relies on visualizing the hyperechoic needle tip, ideally with the needle bevel facing the ultrasound probe. Moving the ultrasound probe along with the needle to track its tip as the vessel is approached is crucial. Continuous visualization of the needle tip is essential because the entire needle may not be visible, unlike in the longitudinal approach. Losing sight of the needle tip can lead to inadvertent puncture of nearby structures or the vessel's back wall. Visibility may be maintained by making slight needle movements and observing tissue movement while gently fanning the probe back and forth until the needle tip is seen.
Once the needle enters the vessel using either approach, it should remain inside until the angiocatheter can be advanced. The longitudinal approach typically offers easier visualization of vessel entry, as both the needle and vessel length are visible on the screen. In the transverse approach, the needle can be advanced by slight movements followed by gently fanning the probe, ensuring the needle tip stays centered in the vessel. These 2 approaches may be used separately or in combination based on the operator's preference and procedural requirements. Some vendors offer multiplanar ultrasound probes that allow simultaneous visualization of the vein's short and long axes, enhancing safety and reducing the risk of catheter misplacement (see Image. Ultrasound Intravenous Access Multiplanar Views).
Procedure
1. Discuss the procedure, including the steps, expected outcomes, risks, benefits, and alternatives. If necessary, obtain consent from the patient.
2. Collect the materials and equipment (see Preparation).
3. Use the high-frequency ultrasound probe to scan desired locations and identify the best access site. Consider relative contraindications, vessel depth, size, shape, and path, and overlying structures such as nerves or other vessels in the same path. The impact the site will have on the patient’s comfort and range of movement must also be anticipated. The optimal needle entry point may be marked at this time if desired.
4. Prepare the site as follows:
- Topical anesthetic: Depending on the individual and situation, consider using a local anesthetic, such as a topical eutectic mixture of lidocaine and prilocaine or a vapocoolant spray.
- Warming: Consider local warming of the site. While used in cases of small vessels or vasoconstriction, this technique has demonstrated improved first-stick success and reduced time to access. Two minutes of heat has been shown to counteract the vasoconstriction occurring after using a eutectic mixture of lidocaine and prilocaine.
- Tourniquet: A tourniquet should be placed 3 to 4 centimeters proximal to the insertion site. The length of the needle used may affect the length of the tourniquet.
- Cleaning the site: The prep pad provided in the central or intravenous line starter kit, steeped in alcohol or another antiseptic, may be used to clean the site.
- Unlocking the needle cap: Most needles have a cap that may be hard to remove one-handed, so it is beneficial to have the needle set up and ready.
- Saline lock: Ensure the saline lock and cap are attached (and preflushed) and that they are easily reached along with the transparent patch and any other securing dressing to be used.
5. Apply Tegaderm or a sterile probe cover, depending on the procedure.
6. Identify the location and vessels with ultrasound, ensuring verification of the vein or artery. Align the targeted vessel centrally with the probe and screen on either the short or long axis (depending on user preference).
7. Advance the needle under real-time ultrasound guidance and observe its insertion into the vessel. Maintain continuous visualization on the screen to avoid losing sight of the needle and vessel position. Check for blood return (eg, "flash") in the hub. Some clinicians prefer visualizing further advancement within the vessel to ensure that the catheter, when advanced off the needle, remains well-positioned within the vessel.
8. Advance the catheter from the needle into the vessel. Withdraw the needle manually or with the needle’s adjunct, as some needles may have a button for spring-loaded needle withdrawal.
9. Draw any blood required for diagnostic purposes.
10. Attach the preflushed syringe to the catheter and secure the site with the dressing(s) chosen. Before dressing, clean any remaining gel from the site; otherwise, adhesive dressings are likely to fail.
11. Remove the tourniquet and flush the tubing to ensure smooth flow and verify the absence of catheter or fluid infiltration. During flushing, repositioning the ultrasound probe on the patient to observe the target vessel can be beneficial. A slight dilation of the vessel often occurs, aiding in confirming proper placement.
12. To confirm the final position within the vein, inject saline into the intravascular line and scan the proximal part of the vein to differentiate tissue infiltration from enhanced flow in the secured vein.
13. Secure the access site with bioocclusive dressing, according to institutional policies. The site must be assessed daily to avoid infection or infiltration.
Complications
Ultrasound-guided intravenous access has no specific complications, unlike the traditional method. Results from a published study suggests that peripheral intravenous catheters placed under ultrasound guidance may fail earlier than expected, with an average life of approximately 26 hours. The shorter functional duration may be due to the patients who require this modality or the individual placing the catheter rather than using the procedure itself.
Clinical Significance
The benefits of ultrasound-guided intravenous access are seen in both adults and children. A primary benefit is the increased success rate, which has been shown multiple times in preidentified subgroups of complex cases and nonselected outpatients. With this success rate, the use of ultrasound for vascular access has been shown to decrease the need for central line placement. Ultrasound guidance leads to an increased first-attempt success rate, a faster time to intravenous access, and higher patient satisfaction.
Enhancing Healthcare Team Outcomes
All healthcare professionals who start peripheral or central lines should be familiar with the use of ultrasonography. This noninvasive technology can be helpful in patients with difficult intravenous access. While not as common, ultrasound can also be used for arterial access and cannulation. Once mastered, the procedure is simple, effective, safe, and presents little to no increased risk or contraindications. Limitations to using ultrasound-guided intravenous access include the availability of ultrasound machines and the required training. Several types of portable ultrasound probes are available and can be sterilized for use on almost any part of the body. However, healthcare professionals need to acquire the skills necessary to effectively use ultrasound.
Nursing, Allied Health, and Interprofessional Team Monitoring
Intravenous access is essential for administering medications, fluids, and nutrients directly into the bloodstream. Proper care and maintenance of intravenous access are crucial to prevent complications such as infections, phlebitis, and infiltration. Attention should be paid to performing hand hygiene, using alcohol-based hand rub, or washing hands with soap and water before and after handling intravenous equipment or accessing intravenous sites.
The aseptic technique must be used during intravenous catheter insertion. The catheter must be adequately secured to minimize movement and prevent dislodgement. The intravenous insertion site must be inspected regularly for signs of infection, infiltration, or phlebitis. Intravenous dressings must be replaced according to hospital policy or if they become wet, soiled, or non-occlusive. The intravenous tubing must be labeled with the date and time of insertion and change. Any signs of complications, such as infection, phlebitis, infiltration, and extravasation, should be promptly identified and addressed. Hospital protocols for managing complications must be implemented, which may include removing the intravenous line, applying warm or cold compresses, and notifying the clinician.
Media
(Click Video to Play)
Forearm Anatomy Review and Ultrasound Probing. This video features a review of forearm anatomy and appropriate arm positioning for locating upper arm veins for ultrasound-guided intravenous access.
Contributed by Bradley Presley, MD
(Click Video to Play)
Ultrasound Assessment for Intravenous Placement. The blue arrow points to a vein, which collapses with gentle pressure from the ultrasound transducer. The red arrow points to an artery, which is less collapsible than a vein.
Contributed by Dr. Vaibhav Bora MBBS, FASE, FASA
(Click Image to Enlarge)
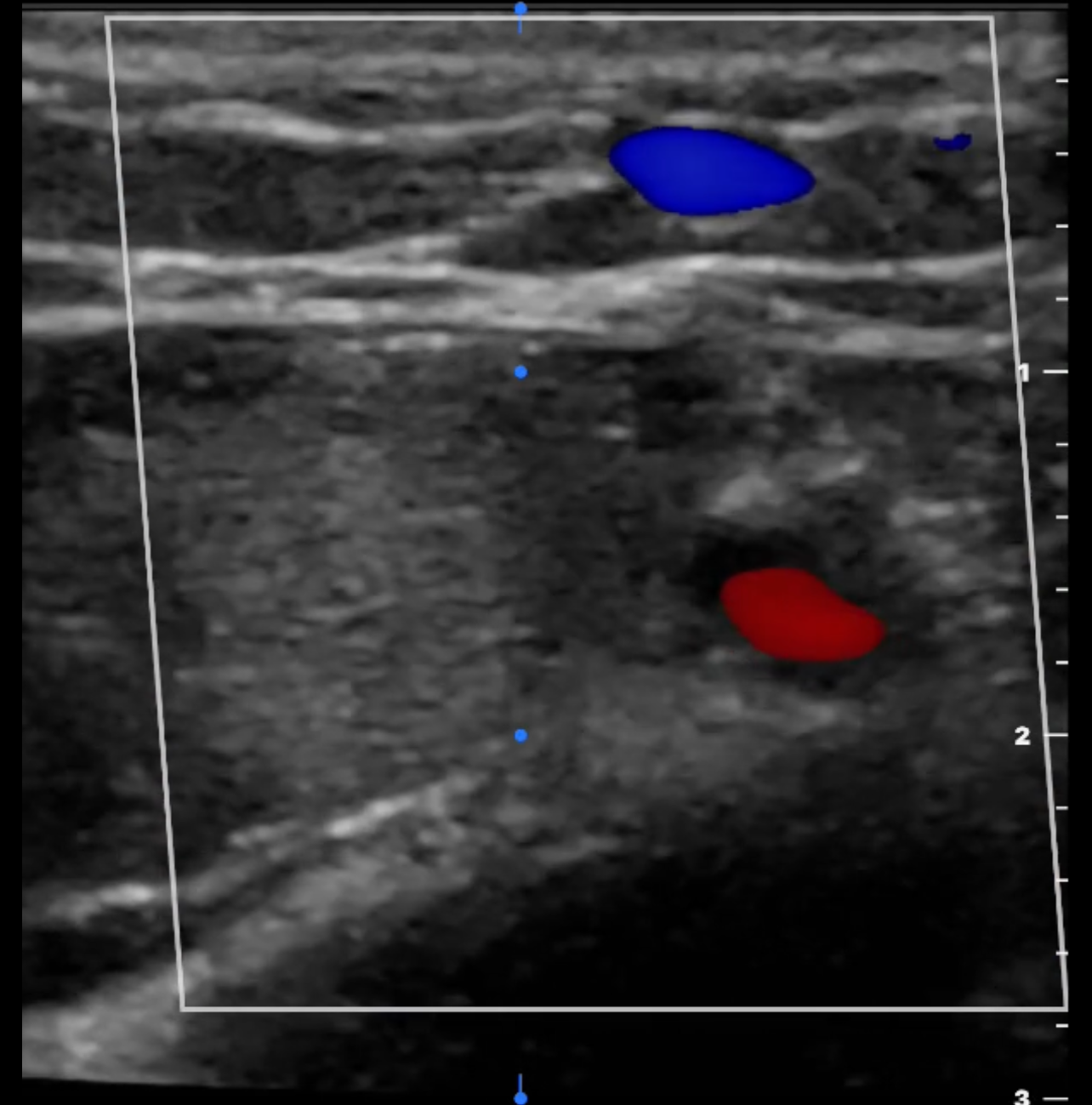
Color Doppler Ultrasound of Artery versus Vein. Color Doppler ultrasound typically shows blood flow in the pulsatile artery as red, indicating blood moving toward the probe. Blood flow in the collapsible vein is depicted in blue, indicating blood moving away from the probe.
Contributed by Dr. Vaibhav Bora MBBS, FASE, FASA, FCCP, FCCM
(Click Image to Enlarge)

Ultrasound Intravenous Access Multiplanar Views. This image shows the simultaneous orthogonal imaging of different blood vessel planes—the short and long axes—to assist in placing and confirming the position of the intravenous catheter during ultrasound-guided intravenous access.
Contributed by Dr. Vaibhav Bora MBBS, FASE, FASA, FCCM, FCCP
References
Kinnaird T, Gallagher S, Cockburn J, Sirker A, Ludman P, de Belder M, Smith E, Anderson R, Strange J, Mamas M, Hildick-Smith D, British Cardiovascular Intervention Society and the National Institute for Cardiovascular Outcomes Research. Procedural Success and Outcomes With Increasing Use of Enabling Strategies for Chronic Total Occlusion Intervention. Circulation. Cardiovascular interventions. 2018 Oct:11(10):e006436. doi: 10.1161/CIRCINTERVENTIONS.118.006436. Epub [PubMed PMID: 30354634]
Samarasena JB, Yu AR, Chang KJ. EUS-guided portal pressure measurement (with videos). Endoscopic ultrasound. 2018 Jul-Aug:7(4):257-262. doi: 10.4103/eus.eus_35_18. Epub [PubMed PMID: 30117489]
Soga Y, Nakamura M, Hirose K, Ito N, Tomoi Y, Hiramori S, Ando K. Primary Use of the TruePath Crossing Device for Infrainguinal Chronic Total Occlusions With Intravascular Ultrasound Evaluation. Journal of endovascular therapy : an official journal of the International Society of Endovascular Specialists. 2018 Oct:25(5):592-598. doi: 10.1177/1526602818793901. Epub 2018 Aug 17 [PubMed PMID: 30117364]
Liu VY, Agha AM, Lopez-Mattei J, Palaskas N, Kim P, Thompson K, Mouhayar E, Marmagkiolis K, Hassan SA, Karimzad K, Iliescu CA. Interventional Cardio-Oncology: Adding a New Dimension to the Cardio-Oncology Field. Frontiers in cardiovascular medicine. 2018:5():48. doi: 10.3389/fcvm.2018.00048. Epub 2018 May 17 [PubMed PMID: 29868614]
Murray TE, O'Neill DC, Lee MJ. Combining Ultrasound-Guided Vascular Access With Ultrasound-Guided Analgesia for Single Skin and Vessel Puncture. Journal of endovascular therapy : an official journal of the International Society of Endovascular Specialists. 2018 Jun:25(3):355-357. doi: 10.1177/1526602818761380. Epub 2018 Mar 12 [PubMed PMID: 29529915]
Francisco ARG, Duarte J, de Oliveira EI. Port-A-Cath Catheter Embolization to Distal Pulmonary Artery Branches: Two Tailored Percutaneous Retrieval Approaches. Vascular and endovascular surgery. 2018 Jul:52(5):361-366. doi: 10.1177/1538574418762191. Epub 2018 Mar 8 [PubMed PMID: 29519203]
Wang D. Image Guidance Technologies for Interventional Pain Procedures: Ultrasound, Fluoroscopy, and CT. Current pain and headache reports. 2018 Jan 26:22(1):6. doi: 10.1007/s11916-018-0660-1. Epub 2018 Jan 26 [PubMed PMID: 29374352]
Weaver JJ, Dobrow EM, Hsu EK, Monroe EJ. Single-access liver floss technique with antegrade hepatic vein access and recanalization in Budd-Chiari syndrome. Diagnostic and interventional radiology (Ankara, Turkey). 2018 Jan-Feb:24(1):38-41. doi: 10.5152/dir.2017.17327. Epub [PubMed PMID: 29187341]
Takahashi Y, Sato T, Okazaki H, Nozaki A, Matsushita M, Kamiya M, Shimizu W. Transvenous Intravascular Ultrasound-Guided Endovascular Treatment for Chronic Total Occlusion of the Infrainguinal Arteries. Journal of endovascular therapy : an official journal of the International Society of Endovascular Specialists. 2017 Oct:24(5):718-726. doi: 10.1177/1526602817723139. Epub 2017 Aug 2 [PubMed PMID: 28766400]