Introduction
The prostate is a "walnut-shaped gland, a part of the male reproductive system that produces and secretes thin alkaline fluid in the ejaculate. It contains glandular and stromal elements that are subject to enlargement and developing adenocarcinoma in an elderly patient. Infection is common in relatively younger patients. Imaging plays a vital role in the diagnosis of different prostatic pathology, including early detection of carcinoma. Imaging also helps obtain tissue samples, drain the abscess and post-procedure collections, and stage and follow malignancy.
Anatomy
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy
The prostate is located in the pelvic cavity inferior to the urinary bladder surrounding the prostatic urethra. The gland comprises an apex resting on the urogenital diaphragm, a base attached to the bladder neck, and inferolateral surfaces resting on the levator ani facia above the urogenital diaphragm. See Image. Median Sagittal Section of Male Pelvis Anatomy. Anatomically, it is divided into 2 lateral (right and left) and one median lobe. Histologically, it has a central zone (CZ) comprising 25% of the prostatic mass that forms the base; a peripheral zone (PZ) surrounding the central part constituting 25% of the prostatic mass; and a transition zone (TZ) that surrounds the anterolateral portion of the urethra in a horseshoe-like fashion. It is essential to know these histological zones because 70% of the adenocarcinomas arise from the peripheral zone while 20% are from the transition zone. Only 10% of adenocarcinomas arise from the central zone. Prostatitis more often occurs in the central zone. Benign prostatic hyperplasia typically expands the transitional zone creating adenoma.
Plain Films
Plain radiographs have limited prostate evaluation utility but are rarely used as a skeletal survey to assess or follow metastases. Other imaging modalities like bone scans are used for assessing bone metastases, and computed tomography (CT) of the chest, abdomen, and pelvis are used to stage prostate cancer. Magnetic resonance imaging (MRI) of the prostate is sensitive and specific for assessing prostate malignancy and local extension. CT/MRI is also used to place radiation seeds before radiotherapy.
Computed Tomography
Detailed prostate anatomy is not well defined on the CT scan, as is its pathology. It may show a hyperdense central zone with density adjusted around 40 to 60 Hounsfield Unit (HU), and the peripheral zone may appear hypodense between 10-5 HU density.
Benign Prostatic Hyperplasia
CT scan is not typically done for diagnosis, but benign prostatic hyperplasia (BPH) is identified when the prostate extends above the pubic symphysis on axial imaging. BPH can also be diagnosed on a CT scan with a volume greater than 30 mL (measured with the help of coronal reformate images).
Prostate Inflammation
In prostatitis, the gland appears diffusely hypodense with symmetric or asymmetric enlargement. Prostatic abscesses are well-defined hypoattenuating (approximately fluid density, around -19 to 13 HU) areas with peripheral rim enhancement. The progression of the disease can be monitored with a CT scan or alternative to sonography.[1]
Prostate CA
Prostatic malignancy appears as contrast-enhancing areas, particularly in the venous phase. These areas can be focal or diffuse and are found within the peripheral zone. CT scan has a role in carcinoma imaging to assess local and distant spread.[2]
Magnetic Resonance
MRI is an excellent modality for prostate imaging due to its better contrast resolution. MRI can differentiate anatomical zones and their abnormalities. Prostate MRI is performed with a pelvic coil and is sensitive in detecting malignancy and assessing its local extension. The use of an endorectal coil provides more information and better resolution (see Image. Normal Prostate, Magnetic Resonance Image Using Endorectal Coil). With recent advances like multiparametric MRI (mp-MRI), functional MRI, and an MRI-guided biopsy, MRI is increasingly useful in detecting low-grade or low-volume prostate carcinoma. Necessary MRI sequences include T2-weighted, diffusion-weighted imaging (DWI) along with an apparent diffusion coefficient (ADC) and dynamic intravenous contrast-enhanced imaging. DWI analyzes the diffusion of water molecules at the cellular level. ADC is a qualitative measure of average water diffusion per voxel. DWI is particularly important in the diagnosis of prostate carcinoma and prostatitis, including abscesses.[3]
Normal Anatomy
The peripheral zone is homogeneously hyperintense on T2 weighted imaging (T2WI) with the hypointense capsule. The transition zone shows heterogeneity while seminal vesicles appear uniformly hyperintense on T2WI.
BPH
MRI delineates zonal anatomy, its elements, and gland volume as well as zonal volume. BPH appears as a heterogenous TZ on T2WI. Due to glandular or stromal tissue enlargement, enlarged nodules in BPH show increased or decreased signals on T2WI. Glandular enlargement appears as bright signals on T2WI, while fibromuscular and stromal elements are dark on T2WI. Estimation of stromal and glandular ratio helps to choose appropriate medical therapy.[4] Stromal enlargement may mimic transitional zone cancer due to low intensity on T2WI, diffusion restriction, and contrast enhancement, similar to prostatic carcinoma. Stromal hyperplasia can be differentiated by having a more well-defined and encapsulated appearance.[5]
On MRI, BPH can be divided into seven types. Type 0= no/little zonal enlargement. Type 2= retrourethral. Type 3= retrourethral+ bilateral TZ. Type 4= pedunculated (multiple or solitary). Type 5= pedunculated + bilateral TZ +/- retrourethral. Type 6= subtrigonal or ectopic enlargement. Type 7= other combinations. Besides diagnosing BPH, MRI plays an important role in identifying carcinoma when a patient with BPH has increased PSA and is suspicious or at high risk for developing prostate cancer.[4]
Prostate Infection
Bacterial prostatitis is acute or chronic and is more common in the peripheral zone. Acute prostatitis appears T2 hyperintense with increased contrast enhancement. Chronic prostatitis is usually hypointense on T2 and shows poor contrast enhancement. Chronic prostatitis demonstrates increased diffuse restriction due to inflammatory cell infiltrate. These findings mimic prostatic carcinoma. However, the degree of diffusion restriction is lower than carcinoma. Non-necrotic granulomatous prostatitis also appears hypointense on T2 with diffusion restriction, but contrary to chronic prostatitis, there is no enhancement on postcontrast imaging. The necrotic area of granulomatous prostatitis shows an increased signal on T2WI. In patients with extra-prostatic extension of the granulomas, it's challenging to differentiate them from carcinomas.[5][6] Prostatitis may progress into abscesses, which is hyperintense on T2, hypointense on T1, and show peripheral contrast enhancement. The abscesses show diffusion restriction and low ADC value.[7]
Prostate Malignancy
Prostate carcinoma is related to high morbidity and mortality worldwide. MRI, especially mp-MRI, is useful for cancer detection and helps to avoid unnecessary biopsy. Pre-biopsy MRI and MRI-guided biopsy is more superior to the transrectal guided ultrasound (TRUS) biopsy.[8] Pre-biopsy MRI helps avoid over-staging errors that may occur due to biopsy artifacts.[9] MRI also detects anterior, lateral, and apex tumors, which may be missed by biopsy. The malignant lesions are typically in the peripheral zone with T2WI hypointensity, focal enhancement, and low diffusivity. Ill-defined and T2 hypointense lesions in PZ are highly suspicious for carcinoma. Though malignancy is less common in the transition zone, non circumscribed, spiculated, relatively T2 hypointense lesions are suspicious.
MRI is also used to assess metastases that are not visualized on the bone scan or CT. It's also used to evaluate pathological fractures and associated complications. PI-RADS- Prostate Imaging Reporting and Data System is a standardized classification based on mp-MRI findings updated in 2015, known as PI-RADS version 2 = PI-RADS™ v2. According to it, the presence of clinically significant carcinoma is categorized into the following:
- PI-RADS 1: Highly unlikely; normal T2WI and diffusion-weighted (DW)/ADC
- PI-RADS 2: Unlikely-circumscribed; heterogeneity on T2WI and hypointensity PZ on DW/ADC (see Image. Magnetic Resonance Image of Prostate, Imaging Reporting and Data System-2 Classification)
- PI-RADS 3: Equivocal-heterogenous lesion with obscured margin on T2WI; hyperintense on DW &andhypointense on ADC (see Image. Magnetic Resonance Image of Prostate, Imaging Reporting and Data System 3 Classification)
- PI-RADS 4: Likely; non circumscribed </= 1.5 cm lesion, moderately homogenously hypointense on T2WI; hyperintensity on DW and hypointense on ADC
- PI-RADS 5: Highly likely; similar to PI-RADS 4 but lesion > 1.5 cm or extra-prostatic extension
Ultrasonography
Ultrasound is widely available for prostate evaluation but also for performing guided prostatic biopsy. Transabdominal (TAUS) or transrectal sonography can be used to evaluate the prostate, and transrectal is preferred for biopsy. See Image. Transrectal Ultrasound Guided Biopsy of the Prostate. The prostate is examined with TAUS by a transducer placed just above the pubic symphysis with a fluid-filled urinary bladder serving as an acoustic window. The average normal measurements are 3.75 to 4.00 × 2.5 to 3.00 × 3.1 to 3.8 cm (width x height x length) with a volume of 20 to 25 cm. The prostate volume is calculated using the formula for measuring any ellipsoidal structure is 0.5236 × height (H) × width (W) × length (L).[10]
TAUS is limited in obese patients, and in those, bladder filling is not possible to correctly evaluate prostate volume. TRUS is performed in such cases. TRUS is also necessary for suspected prostatic pathology during the clinical exam, increased prostate-specific antigen (PSA) in the blood serum, prostatic inflammation/abscess, and follow-up of prostatic cancer, as TRUS allows detailed evaluation of the prostate.
For TRUS, an endorectal transducer having a frequency of 8 to 10 MHz is delicately inserted into the rectum. Prostate volume is measured similarly to TRAS by obtaining width, height, and length. The gland is evaluated for its shape, symmetry, echogenicity, and integrity of the prostatic capsule. Periprostatic structures, e.g., seminal vesicles, neurovascular bundles, and blood vessels, are assessed for any abnormality, especially in suspected prostate carcinoma.[11] Elastography is a vital aid performed during TRUS to evaluate the firmness of the prostate tissue. The areas of increased firmness are often identified on elastography, which does not show any abnormal echogenicity on grayscale imaging.
Benign Prostatic Hyperplasia
TAS OR TRUS assesses the prostate volume to determine the course of management, ie, prostatic volume more than 80 cm3 qualifies for open surgery-adenomectomy; otherwise, transurethral resection is the choice for management. European Association of Urology (EAU) suggests measuring prostatic volume via TRUS and residual urinary bladder post-void urine volume through TAUS. Ultrasound examination should be supplemented by visualization of the upper urinary tract to assess the degree of urinary tract dilatation.
Prostate Inflammation
Prostatitis is usually a clinical diagnosis. Sonography in prostatitis frequently demonstrates an enlarged and/or deformed gland with inhomogenous echotexture. Acute prostatitis may result in a parenchymal abscess, which appears as a hypoechoic or fluid consistency lesion within the prostate parenchyma. Ultrasound is performed not only for diagnosis but also for planning to evacuate it under ultrasound guidance. Ultrasound is useful in intraprostatic antibiotic injections in chronic prostatitis when pain is exacerbating.[12]
Prostatic Neoplasm
Prostatic malignancy is difficult to diagnose in the USG as the tumor is often isoechoic to the surrounding normal gland. It could be hypoechoic. The ultrasound with color Doppler or power Doppler can identify angiogenesis, showing dilated and tortuous vessels, but it cannot detect small tumor foci. The diagnostic value of ultrasound is around 30% to 40%.[11] Therefore, it's mostly used as a guidance for prostatic biopsy. It is proven to improve cancer detection, especially in men who have a positive PSA and PSA ratio.[13] The ultrasound (US) is often helpful in identifying local tumor spread and thus staging cancer.
Some advances, like elastography, identify consistency differences and help in tumor diagnosis and guided biopsy. On elastography, neoplasm consistency appears firmer than the surrounding normal tissue. 3-dimensional TRUS allows computer processing of sectional images of the prostate and adds more detailed information about the morphology, surrounding structures, etc.[11] The contrast-enhanced US has a high sensitivity to differentiate neoplasm from normal prostate tissue and is more useful for US-guided biopsies.[14]
Nuclear Medicine
Nuclear medicine plays a role in the diagnosis, staging/re-staging, and therapy of prostate carcinoma. Skeletal metastases can be identified with a bone scan. Positron emission tomography (PET) is an examination that assesses malignant activity and its spread in the body. In particular, choline derivative radiotracer, 18F-fluorocholine (F-FCH), is the currently used tracer for diagnosing prostate carcinoma. PET, when combined with CT (PET/CT) and MRI (PET/MRI), adds metabolic/functional data derived from PET to CT or MRI findings.[15][16] Prostate-specific membrane antigen (PSMA) is expressed on the cell surface of carcinoma, nodal metastasis, and metastases to the bones. Ga-labeled PSMA inhibitor is a widely used PET tracer and is now becoming popular, not only for diagnosis but also for therapy.[16]
Angiography
Angiography can be utilized for prostatic artery embolization in patients with BPH and bleeding. It is an interventional technique for managing patients with lower urinary tract symptoms secondary to benign prostatic hyperplasia. Prostatic artry embolization improves lower urinary tract symptoms.
Clinical Significance
Prostate imaging plays a vital role in identifying various pathologies, including infection, enlargement, and carcinoma. It is crucial in staging the carcinoma. PI-RADS is a standardized classification based on MRI findings, which helps in further management. US or MRI-guided procedures are also widely used for diagnosis as well as therapy.
Media
(Click Image to Enlarge)
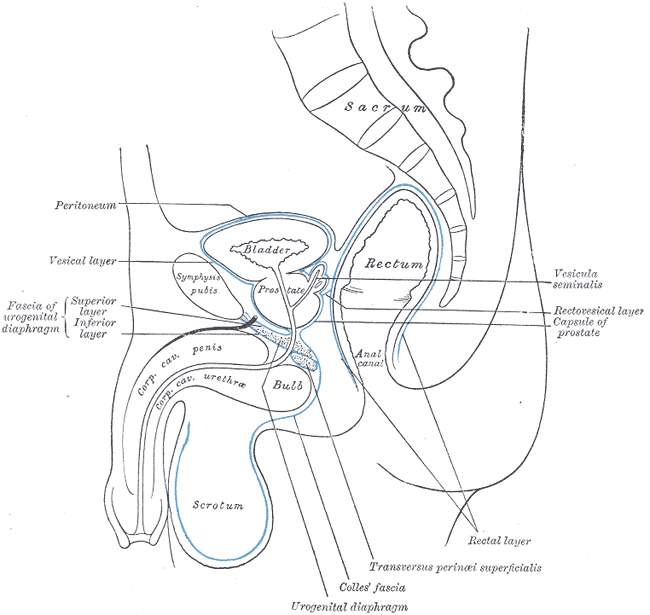
Median Sagittal Section of Male Pelvis Anatomy. Anatomy includes pelvis, sacrum, peritoneum, vesical layer, fascia of urogenital diaphragm, superior and inferior layer, bladder, prostate, symphysis pubis, rectum, anal canal, corpus cavernosum penis and urethra, bulb, scrotum, urogenital diaphragm, Colles fascia, transversus perinei superficialis, rectal layer, vesicula seminalis, rectovesical layer, and capsule of prostate.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
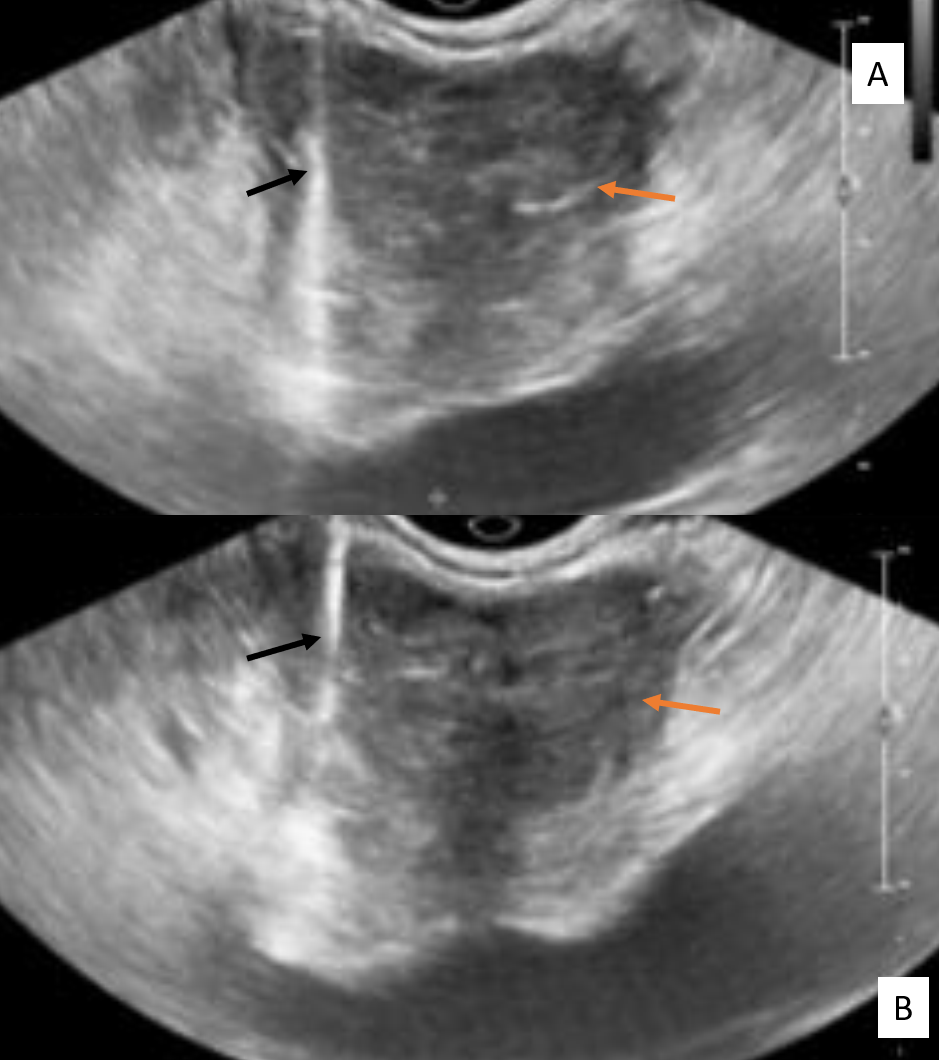
Transrectal Ultrasound Guided Biopsy of the Prostate. The orange arrows point to the prostate. The black arrows point to the biopsy needle.
Contributed by S Walunj, MD
(Click Image to Enlarge)
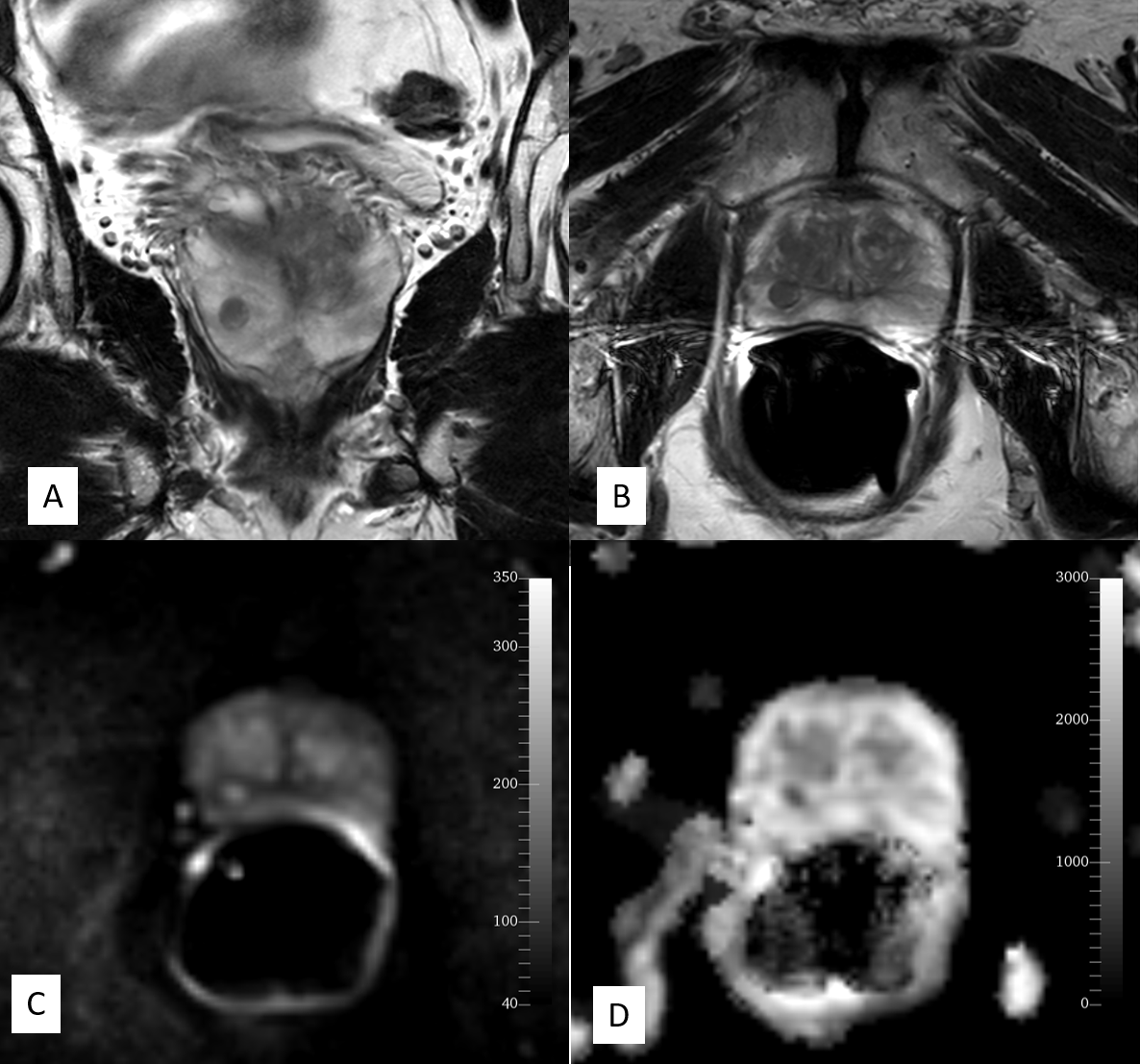
Normal Prostate, Magnetic Resonance Image Using Endorectal Coil. This image is of a normal prostate using an endorectal coil (black coil in the rectum). (A) Ccoronal T2, (B) Axial T2, (C) Diffusion-weighted image, (D) Apparent diffusion coefficient.
Contributed by R Jones, DE, PhD, MBA
(Click Image to Enlarge)
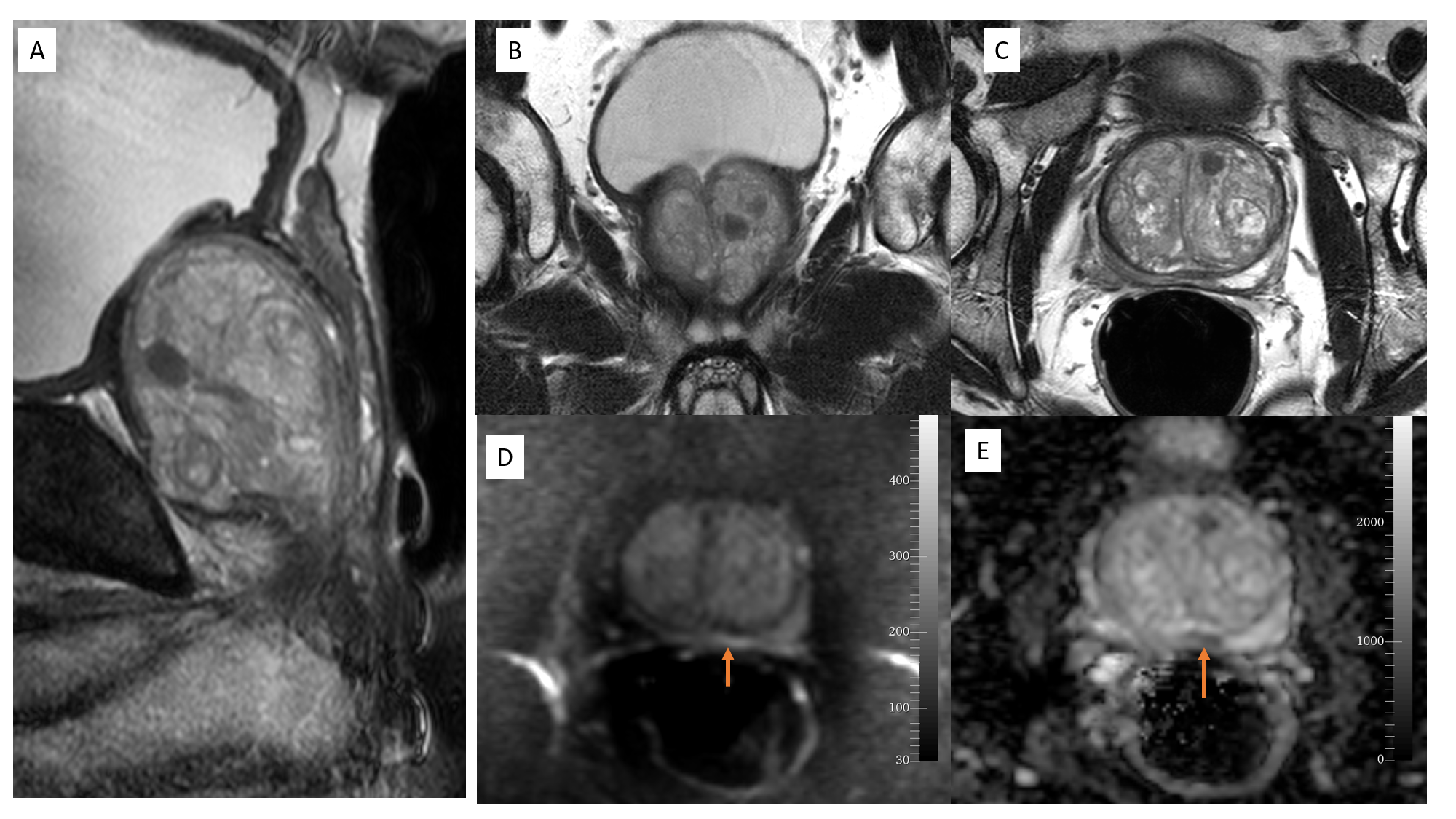
Magnetic Resonance Image of Prostate, Imaging Reporting and Data System-2 Classification. This image shows (A) Sagittal T2, (B) Coronal T2, (C) Axial T2, (D) Difussion-weighted (E) Apparent diffusion coefficient. An ill-defined lesion in the peripheral zone shows faint hyperintensity on DW and is suppressed faintly on ADC (restricted diffusion).
Contributed by R Jones, DE, PhD, MBA
(Click Image to Enlarge)
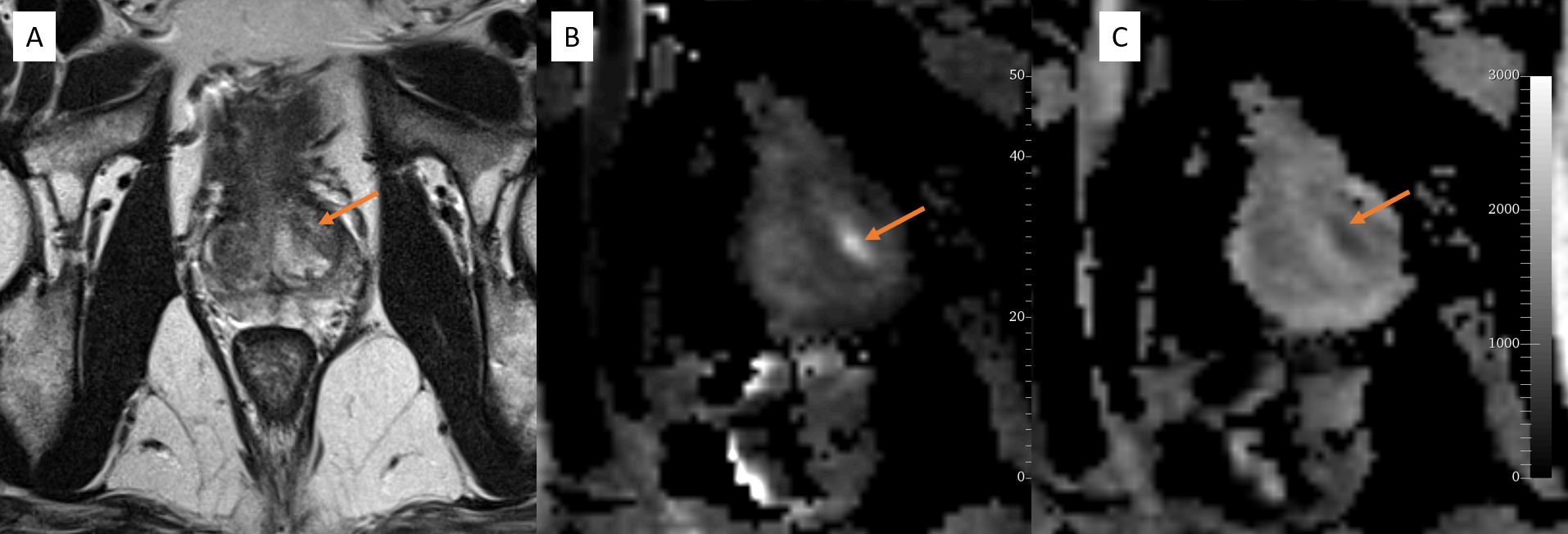
Magnetic Resonance Image of Prostate, Imaging Reporting and Data System 3 Classification. This image shows (A) Axial T2, (B) Diffusion-weighted, (C) Apparent diffusion; the focal area of T2 hypointensity shows faint diffusion restriction (orange arrow).
Contributed by R Jones, DE, PhD, MBA
References
Thornhill BA, Morehouse HT, Coleman P, Hoffman-Tretin JC. Prostatic abscess: CT and sonographic findings. AJR. American journal of roentgenology. 1987 May:148(5):899-900 [PubMed PMID: 3554922]
Jia JB, Houshyar R, Verma S, Uchio E, Lall C. Prostate cancer on computed tomography: A direct comparison with multi-parametric magnetic resonance imaging and tissue pathology. European journal of radiology. 2016 Jan:85(1):261-267. doi: 10.1016/j.ejrad.2015.10.013. Epub 2015 Oct 24 [PubMed PMID: 26526901]
Stabile A, Giganti F, Emberton M, Moore CM. MRI in prostate cancer diagnosis: do we need to add standard sampling? A review of the last 5 years. Prostate cancer and prostatic diseases. 2018 Nov:21(4):473-487. doi: 10.1038/s41391-018-0071-8. Epub 2018 Aug 13 [PubMed PMID: 30104656]
Guneyli S,Ward E,Thomas S,Yousuf AN,Trilisky I,Peng Y,Antic T,Oto A, Magnetic resonance imaging of benign prostatic hyperplasia. Diagnostic and interventional radiology (Ankara, Turkey). 2016 May-Jun; [PubMed PMID: 27015442]
Kitzing YX, Prando A, Varol C, Karczmar GS, Maclean F, Oto A. Benign Conditions That Mimic Prostate Carcinoma: MR Imaging Features with Histopathologic Correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2016 Jan-Feb:36(1):162-75. doi: 10.1148/rg.2016150030. Epub 2015 Nov 20 [PubMed PMID: 26587887]
Bour L, Schull A, Delongchamps NB, Beuvon F, Muradyan N, Legmann P, Cornud F. Multiparametric MRI features of granulomatous prostatitis and tubercular prostate abscess. Diagnostic and interventional imaging. 2013 Jan:94(1):84-90. doi: 10.1016/j.diii.2012.09.001. Epub 2012 Oct 15 [PubMed PMID: 23079151]
Singh P, Yadav MK, Singh SK, Lal A, Khandelwal N. Case series: Diffusion weighted MRI appearance in prostatic abscess. The Indian journal of radiology & imaging. 2011 Jan:21(1):46-8. doi: 10.4103/0971-3026.76054. Epub [PubMed PMID: 21431033]
Level 3 (low-level) evidenceKasivisvanathan V,Rannikko AS,Borghi M,Panebianco V,Mynderse LA,Vaarala MH,Briganti A,Budäus L,Hellawell G,Hindley RG,Roobol MJ,Eggener S,Ghei M,Villers A,Bladou F,Villeirs GM,Virdi J,Boxler S,Robert G,Singh PB,Venderink W,Hadaschik BA,Ruffion A,Hu JC,Margolis D,Crouzet S,Klotz L,Taneja SS,Pinto P,Gill I,Allen C,Giganti F,Freeman A,Morris S,Punwani S,Williams NR,Brew-Graves C,Deeks J,Takwoingi Y,Emberton M,Moore CM, MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. The New England journal of medicine. 2018 May 10; [PubMed PMID: 29552975]
van der Leest M, Israël B, Cornel EB, Zámecnik P, Schoots IG, van der Lelij H, Padhani AR, Rovers M, van Oort I, Sedelaar M, Hulsbergen-van de Kaa C, Hannink G, Veltman J, Barentsz J. High Diagnostic Performance of Short Magnetic Resonance Imaging Protocols for Prostate Cancer Detection in Biopsy-naïve Men: The Next Step in Magnetic Resonance Imaging Accessibility. European urology. 2019 Nov:76(5):574-581. doi: 10.1016/j.eururo.2019.05.029. Epub 2019 Jun 2 [PubMed PMID: 31167748]
Guideline developed in collaboration with the American College of Radiology, Society of Radiologists in Ultrasound. AIUM Practice Guideline for the Performance of an Ultrasound Evaluation of the Prostate (and Surrounding Structures). Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2015 Aug:34(8):1-6. doi: 10.7863/ultra.34.8.15.13.0004. Epub [PubMed PMID: 26206816]
Level 1 (high-level) evidenceTyloch JF, Wieczorek AP. The standards of an ultrasound examination of the prostate gland. Part 1. Journal of ultrasonography. 2016 Dec:16(67):378-390. doi: 10.15557/JoU.2016.0038. Epub 2016 Dec 30 [PubMed PMID: 28138409]
Tyloch JF, Wieczorek AP. The standards of an ultrasound examination of the prostate gland. Part 2. Journal of ultrasonography. 2017 Mar:17(68):43-58. doi: 10.15557/JoU.2017.0007. Epub 2017 Mar 31 [PubMed PMID: 28439429]
Stamatiou K, Alevizos A, Karanasiou V, Mariolis A, Mihas C, Papathanasiou M, Bovis K, Sofras F. Impact of additional sampling in the TRUS-guided biopsy for the diagnosis of prostate cancer. Urologia internationalis. 2007:78(4):313-7 [PubMed PMID: 17495488]
Taymoorian K, Thomas A, Slowinski T, Khiabanchian M, Stephan C, Lein M, Deger S, Lenk S, Loening SA, Fischer T. Transrectal broadband-Doppler sonography with intravenous contrast medium administration for prostate imaging and biopsy in men with an elevated PSA value and previous negative biopsies. Anticancer research. 2007 Nov-Dec:27(6C):4315-20 [PubMed PMID: 18214038]
Anand SS, Singh H, Dash AK. Clinical Applications of PET and PET-CT. Medical journal, Armed Forces India. 2009 Oct:65(4):353-8. doi: 10.1016/S0377-1237(09)80099-3. Epub 2011 Jul 21 [PubMed PMID: 27408291]
Cuccurullo V, Di Stasio GD, Mansi L. Nuclear Medicine in Prostate Cancer: A New Era for Radiotracers. World journal of nuclear medicine. 2018 Apr-Jun:17(2):70-78. doi: 10.4103/wjnm.WJNM_54_17. Epub [PubMed PMID: 29719480]