 Neuroanatomy, Anterior White Commissure
Neuroanatomy, Anterior White Commissure
Introduction
The anterior or ventral white commissure is a collection of nerve fibers that cross the midline of the spinal cord and transmit information from or to the contralateral side of the brain. It is present throughout the length of the spinal cord and lies behind the anterior median fissure. Among the important pathways that decussate in the spinal cord via the anterior white commissure are the second-order neurons of the spinothalamic tract and the upper motor neurons of the anterior corticospinal tract. These crossing fibers make the anterior white commissure an important link in communication between the brain and the contralateral side of the body for both sensory and motor pathways.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
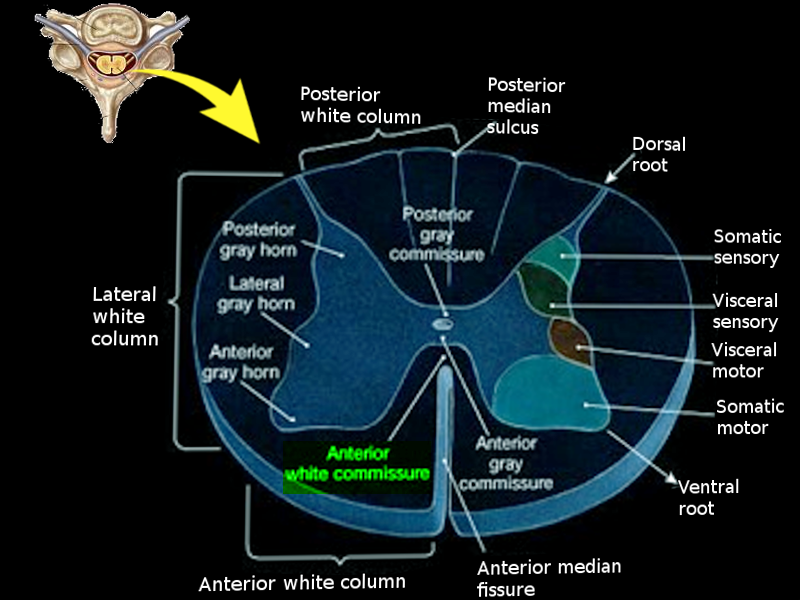
A cross-section of the spinal cord shows a butterfly-shaped area of gray matter composed of nerve cell bodies surrounded by white matter composed of myelinated nerve fibers. The anterior white commissure is a rectangularly-shaped collection of nerve fibers located directly anterior to the central canal and gray commissure, posterior to the anterior median fissure. Sensory fibers from the spinothalamic tract and motor fibers from the anterior corticospinal tract decussate in the anterior white commissure. The anterior white commissure is particularly important in the relay of contralateral sensory and motor information because of these crossing fibers.
The spinothalamic tract is a major ascending neural pathway in the sensory detection of pain, temperature, touch, and pressure. Sensory fibers synapse on cell bodies in the dorsal root ganglion. These axons of second-order neurons from the spinothalamic tract cross over at the anterior white commissure and also ascend one to three levels in the spinal cord through the Lissauer tract. After decussating, they ascend and synapse in the ventroposterolateral (VPL) nucleus of the thalamus. Third-order neurons continue to transmit sensory information to the primary somatosensory cortex.[1]
The corticospinal tract is a major descending neural pathway for the control of voluntary movement. Most of the fibers of the corticospinal tract decussate in the medulla and form the lateral corticospinal tract. Up to 15% of fibers within the anterior corticospinal tract, however, cross at the anterior white commissure. These fibers then synapse with cell bodies of lower motor neurons in the gray matter of the contralateral ventral horn.[2] The anterior corticospinal tract communicates with lower motor neurons that innervate the axial muscles of the trunk.
Embryology
At approximately week three following fertilization, the developing embryo forms the neural groove, the shallow median indentation of the neural plate. The neural tube on the neural plate's lateral margins begins to elevate before joining to form the neural tube. Signaling from the notochord causes the neural tube and related structures to give rise to central nervous system components. The brain arises from the cranial end of the neural tube the spinal cord from the caudal end. Neural crest cells arise from the neural ectoderm during the neurulation process, transitioning from epithelial to mesenchymal cells then migrating and giving rise to the peripheral nervous system.[3][4][5] The anterior white commissure develops as part of the central nervous system and is composed of the white matter of the spinal cord, with embryological derivation from the neuroectoderm.
Blood Supply and Lymphatics
Blood supply to the spinal cord comes from three main vessels: the anterior spinal artery and the two paired posterior spinal arteries.[6] The anterior spinal artery originates from the vertebral artery and from radicular arteries, the most important of which is known as the artery of Adamkiewicz. The anterior spinal artery provides blood supply to the anterior white commissure.
Physiologic Variants
Physiological variations of the anterior white commissure are dependent on the differences between the spinothalamic and anterior corticospinal tracts. Variations among these tracts may result in more or fewer fibers from each respective tract crossing at the anterior white commissure. The anterior corticospinal tract has significant physiological variations between individuals. In a study of 50 spinal cords, 74% had variations in the size of the right and left corticospinal tracts, with most cords having more fibers on the right.[7] Also, the anterior corticospinal tract develops later than the lateral corticospinal tract and may even be absent in certain individuals.[8] As a result, crossing fibers in the anterior white commissure may lack anterior corticospinal tract fibers between individuals.
Surgical Considerations
Commissural myelotomy is a surgical procedure in which an incision is made in the anterior white commissure to interrupt the spinothalamic tract. This procedure aims to interrupt the pain transmission from the spinothalamic tract and leads to bilateral loss of pain. In a study of 11 patients, it was documented to significantly improve pain in 8 patients with oncogenic pain in the abdominal and pelvic regions[9]. Punctate myelotomy (limited myelotomy) is another option to interrupting the nociceptive pathway. Instead of incising the anterior white commissure, the visceral nociceptive signals are interrupted through an incision in the ventromedial dorsal columns of the spinal cord.[10]
Clinical Significance
The anterior white commissure is a clinically important region for central cord syndrome,[11] an incomplete injury that typically involves the cervical spinal cord and affects the upper more than lower extremities. Central cord syndrome can result from acute-on-chronic trauma from falls or motor vehicle collisions, especially among patients over age 50.[12] Syringomyelia, or cavitation of the cervical spinal cord originating in the central canal, begins by affecting crossing spinothalamic fibers of the anterior white commissure, causing a characteristic loss of pain and temperature sensation. Symptoms may progress to a "cape-like" distribution of numbness and weakness as surrounding structures become involved. Because it contains crossing pain and temperature fibers of the spinothalamic tract, the anterior white commissure is also a potential therapeutic target for pain control interventions.
Other Issues
The anterior white commissure of the spinal cord is not to be confused with another midline neural pathway with a similar-sounding name, the anterior commissure of the brain. This latter structure is a fiber bundle running posterior to the corpus callosum that is believed to be important in interhemispheric communication within the brain.[13]
Disclaimer: This scholarly activity was supported (in whole or part) by HCA and/or an HCA-affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA or any of its affiliated entities.
Media
(Click Image to Enlarge)
Anterior white commissure Image courtesy O.Chaigasame
References
Al-Chalabi M, Reddy V, Gupta S. Neuroanatomy, Spinothalamic Tract. StatPearls. 2023 Jan:(): [PubMed PMID: 29939601]
Natali AL, Reddy V, Bordoni B. Neuroanatomy, Corticospinal Cord Tract. StatPearls. 2023 Jan:(): [PubMed PMID: 30571044]
Butler SJ, Bronner ME. From classical to current: analyzing peripheral nervous system and spinal cord lineage and fate. Developmental biology. 2015 Feb 15:398(2):135-46. doi: 10.1016/j.ydbio.2014.09.033. Epub 2014 Oct 24 [PubMed PMID: 25446276]
Level 3 (low-level) evidenceO'Rahilly R, Müller F. Significant features in the early prenatal development of the human brain. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2008:190(2):105-18. doi: 10.1016/j.aanat.2008.01.001. Epub 2008 Jan 29 [PubMed PMID: 18356030]
Elshazzly M, Lopez MJ, Reddy V, Caban O. Embryology, Central Nervous System. StatPearls. 2023 Jan:(): [PubMed PMID: 30252280]
Dommisse GF. The blood supply of the spinal cord. A critical vascular zone in spinal surgery. The Journal of bone and joint surgery. British volume. 1974 May:56(2):225-35 [PubMed PMID: 4854669]
Nathan PW, Smith MC, Deacon P. The corticospinal tracts in man. Course and location of fibres at different segmental levels. Brain : a journal of neurology. 1990 Apr:113 ( Pt 2)():303-24 [PubMed PMID: 2328407]
Jin ZW, Cho KH, Jang HS, Abe H, Murakami G, Rodriguez-Vazquez JF. Anterior Corticospinal Tract Revisited: A Study Using Human Fetuses. Pediatric neurosurgery. 2016:51(3):121-6. doi: 10.1159/000442421. Epub 2016 Feb 13 [PubMed PMID: 26870953]
Viswanathan A, Burton AW, Rekito A, McCutcheon IE. Commissural myelotomy in the treatment of intractable visceral pain: technique and outcomes. Stereotactic and functional neurosurgery. 2010:88(6):374-82. doi: 10.1159/000319041. Epub 2010 Oct 15 [PubMed PMID: 20948242]
Level 2 (mid-level) evidenceHong D, Andrén-Sandberg A. Punctate midline myelotomy: a minimally invasive procedure for the treatment of pain in inextirpable abdominal and pelvic cancer. Journal of pain and symptom management. 2007 Jan:33(1):99-109 [PubMed PMID: 17196911]
Nowak DD, Lee JK, Gelb DE, Poelstra KA, Ludwig SC. Central cord syndrome. The Journal of the American Academy of Orthopaedic Surgeons. 2009 Dec:17(12):756-65 [PubMed PMID: 19948700]
Aito S, D'Andrea M, Werhagen L, Farsetti L, Cappelli S, Bandini B, Di Donna V. Neurological and functional outcome in traumatic central cord syndrome. Spinal cord. 2007 Apr:45(4):292-7 [PubMed PMID: 16773038]
Level 2 (mid-level) evidencevan Meer N, Houtman AC, Van Schuerbeek P, Vanderhasselt T, Milleret C, Ten Tusscher MP. Interhemispheric Connections between the Primary Visual Cortical Areas via the Anterior Commissure in Human Callosal Agenesis. Frontiers in systems neuroscience. 2016:10():101. doi: 10.3389/fnsys.2016.00101. Epub 2016 Dec 26 [PubMed PMID: 28082873]