Introduction
The Rule of Nines, also known as the Wallace Rule of Nines, is a tool utilized by medical providers to assess the total body surface area (TBSA) involved in burn patients. The measurement of the initial burn surface area is important in estimating fluid resuscitation requirements, as patients with severe burns will have insensible fluid losses due to loss of the skin barrier. Moreover, an accurate assessment provides data that will assist in determining the patient's eventual outcomes. Both inadequate estimates and overestimation have their own shortcomings, as under-resuscitation can lead to progressive shock and, ultimately, end-organ damage, and excessive resuscitation places the patient at risk for developing acute respiratory distress syndrome and abdominal compartment syndrome.[1]
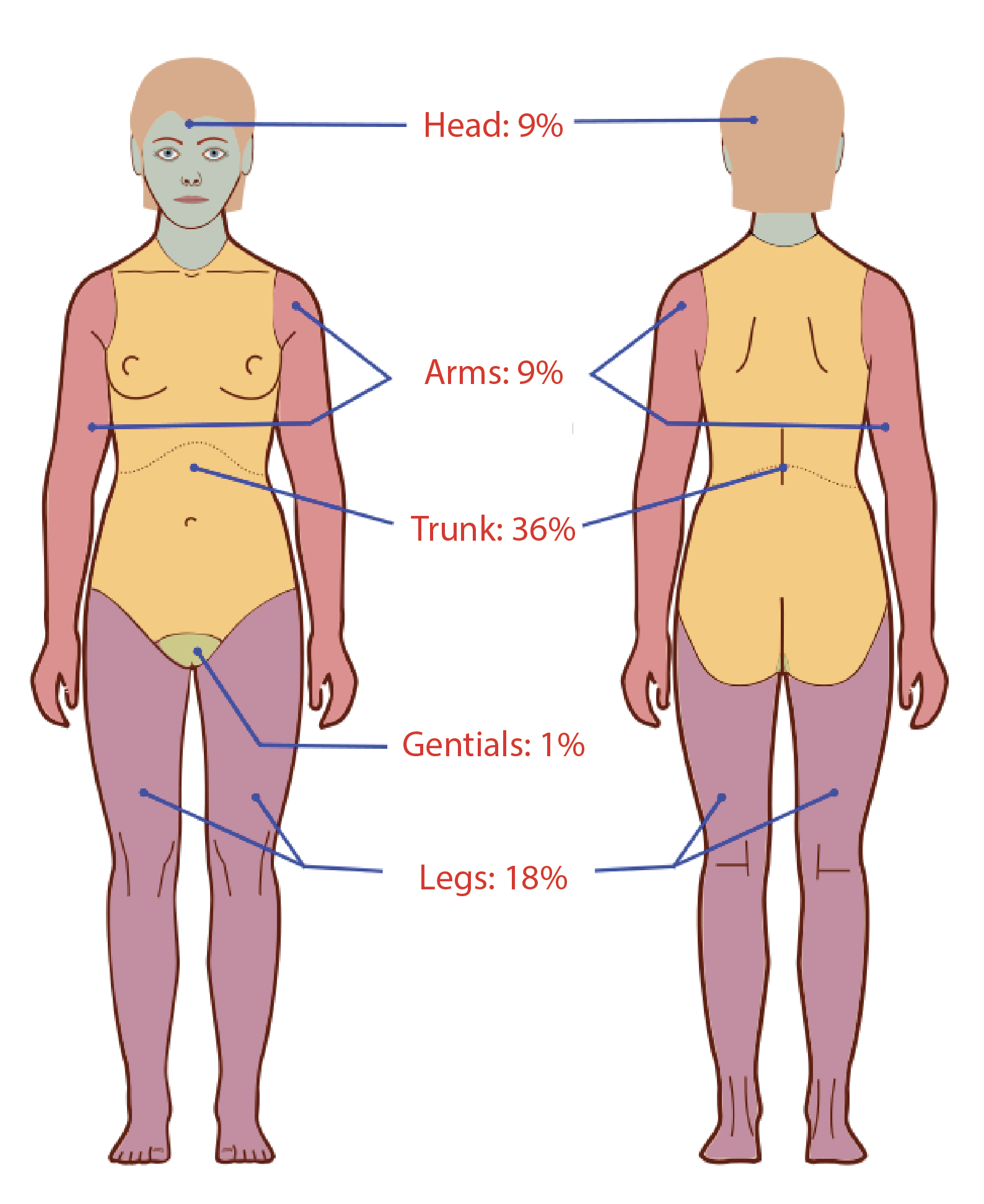
The Rule of Nines was first discussed by Pulaski and Tennison in 1949 and later presented at the National Burns Research Council at a symposium; in 1951, A.B. Wallace published an article in the Lancet in describing the Rule of Nines.[2][3] The Rule of Nines estimation of body surface area burned is based on assigning percentage estimates to different body areas.
- The entire head: 9% (4.5% for anterior and posterior)
- The entire trunk: 36% (can be further broken down into 18% for the anterior torso and 18% for the posterior torso)
- The anterior aspect of the trunk: Can further be divided into the chest and abdomen, each representing 9%
- The upper extremities: 18% (includes 9% for each upper extremity)
- Each upper extremity: Can be further divided into its respective anterior and posterior portions (4.5% each).
- The lower extremities: 36% (18% for each); can be further divided into 9% for the anterior and 9% for the posterior aspect
- The groin: 1% [4][5]
Only second- and third-degree burns, more commonly referred to as partial- and full-thickness burns, respectively, are included in the determination of the TBSA. This method aids hospital and prehospital providers in making a quick assessment to determine the severity, indications for intravenous fluid resuscitation, and the need for transfer to a certified burn center.[2][6][2] Age and body mass index (BMI) are several factors that may affect changes to the Rule of Nines.[7][8][9]
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
The Rule of Nines assesses the proportion of body surface area with partial- and full-thickness burns. Partial-thickness burns affect the epidermis and the papillary or reticular dermis or both layers. These patients present with painful burns, unroofed or intact blisters, and either a homogenous pink/red wound bed if superficial or a slightly mottled wound bed if deeper. Full-thickness burns extend beyond the dermis, are often insensate, and have a charred or leather-like appearance.[2] Once the TBSA is determined and the patient is weighed in kilograms, the amount of fluid resuscitation is calculated using several formulas if the adult patient has more than 20% TBSA.
Fluid resuscitation is paramount as the injured skin allows for insensible losses, and vascular permeability increases, which causes fluid to migrate into interstitial space.[10] The most commonly used formulas include the Parkland and the modified Brooke formula. The Parkland formula was developed in 1968 by Baxter and Shire and calculates the 24-hour resuscitation requirements for large TBSA using 4 mL of crystalloid intravenous fluids per kilogram of body weight per TBSA percent burned. Due to concerns of over-resuscitation, the modified Brooke formula emerged to assist in eliminating the consequences in multiple organ systems associated with excess fluid administration. The modified Brooke formula uses 2 mL of crystalloid instead of the 4 mL described in the Parkland formula.[11]
After the total volume of intravenous fluid resuscitation for the first 24 hours is established, the first half of the volume is given over the first 8 hours, and the remainder is administered over the next 16 hours. The hourly fluid rate is determined by dividing half the total volume by 8 and 16 hours, respectively. The marked start time of fluid resuscitation begins at the time of the burn injury. Should the patient present 2 hours after sustaining the burn and intravenous fluid resuscitation has not been started, the first half of the volume should be given in the next 6 hours. However, if intravenous fluids were administered before arrival, this amount of fluid should be accounted for in the total amount of fluids required.
Colloids are not recommended during the first 8 hours after burn injury as the damage to the endothelial barrier does not limit intravascular fluid losses. Ultimately, the use of colloids can reduce resuscitative volumes and limit over-resuscitation.[12] Resuscitative fluids should be titrated to maintain a goal urine output greater than 0.5 mL per kilogram per hour (30 mL per hour) for adults and children over 30 kg and greater than 1 mL per kilogram of body weight per hour in children below 30 kg.[12][13] Proper fluid resuscitation is key in determining a patient's mortality and risk of complications during the acute initial phase of injury. An unbalanced resuscitation places the patient at risk for developing end-organ damage if the patient is under-resuscitated or pulmonary edema and abdominal compartment syndrome with over-resuscitation.[1][14][15]
Issues of Concern
There is a concern among clinicians about the accuracy of the Rule of Nines given the varying nature of provider subjectivity, especially for assessments within larger body regions.[16] This concept becomes more problematic when determining TBSA in obese and pediatric populations. The discrepancy in TBSA becomes even more apparent when calculated by less experienced providers.[8] The shortcoming of TBSA assessment is not a novel concept and has been well-documented since the 1980s.[17]
Nevertheless, the Rule of Nines provides the most accurate estimations of TBSA patients greater than 10 kg and less than 80 kg. Unfortunately, the Rule of Nines assumes all adults have the same distribution of body surface area percentages regardless of their varying weight, height, and body shapes.[1][18] A patient's BMI is internationally recognized as the most commonly used criterion for defining obesity.[10] For obese and pediatric patients, special consideration should be taken.
Obese Patients
- The obesity epidemic is ongoing in the United States, with rates increasing from 2-fold up to 7-fold and continuing to rise.
- Patients defined as obese by BMI, with a BMI over 30, have disproportionately larger trunks than their nonobese counterparts.
- Obese patients have a closer approximation to 50% TBSA of the trunk, 15% TBSA for each leg, 7% TBSA for each arm, and 6% TBSA for the head.
- Android-shaped patients, defined as a preferential trunk and upper body distribution of adipose tissue (abdomen, chest, shoulders, and the nape of the neck), have a torso closer to 53% TBSA.
- Gynecoid-shaped patients, defined as a preferential lower body distribution of adipose tissue (lower abdomen, pelvis, and thighs), have a torso closer to 48% TBSA.
- Burns on the extremities are significantly overestimated compared to burns on the torso in this population.
- The "Rule of Fives" has been proposed by Livingston et al. to overcome the inaccuracies of estimating TBSA in obese patients, given that more than 50% of TBSA is contributed by the trunk. This formula assigns each arm 5% TBSA, each leg 20%, and 50% for the trunk.
- TBSA may be underestimated in women with larger breasts with burns to the anterior torso. For every increase in breast cup size, there is a subsequent increase by a factor of 0.1 compared to the posterior torso.
- Increasing weight has been associated with lower fluid resuscitation and higher mortality rates.[1][10][19][20]
Pediatric Patients
- Pediatric physiology differs from adults with smaller circulating blood volumes, greater surface area to mass ratio, thinner skin, and different body proportions throughout the various age groups.
- Infants and younger children have proportionately larger heads, altering the surface area distribution of other major body segments.
- The Lund and Browder paradigm accounts for the varying proportions during human growth, which allows for more accurate TBSA calculation in children.
- A "Rule of Eights" has been proposed as a better TBSA estimate for patients weighing less than 10 kg. This rule dictates approximately 32% TBSA for the patient's trunk, 20% TBSA for the head, 16% TBSA for each leg, and 8% TBSA for each arm.[20][21][20][22]
Despite the efficiency of the Rule of Nines and its penetrance into the surgical and emergency medicine specialties, studies show that at 25% TBSA, 30% TBSA, and 35% TBSA, the percentage TBSA is overestimated by 20% when compared with computer-based applications. Overestimation of TBSA burned can lead to excessive intravenous fluid resuscitation giving the potential for volume overload and pulmonary edema with more cardiac demand. These effects can be further exacerbated if fluid resuscitation is strictly determined using the resuscitation formulas without considering the patient's individual and burn characteristics.[17]
Patients with pre-existing comorbidities are at risk for acute cardiac and respiratory decompensation and should be monitored in the intensive care unit (ICU) during the aggressive fluid resuscitation phase, preferably in a burn center.[23][24] Burns can also convert to deeper or more widespread burns as time progresses, which can alter the TBSA estimation.[25]
Clinical Significance
The Rule of Nines is a simple and time-efficient tool used to determine the initial management of resuscitation in larger burned patients. Once the patient's clothing is removed, their TBSA percentage can be defined in a few minutes with the proper resources. On the other hand, the Rule of Palms can be more beneficial in smaller burns. The affected areas are measured using the patient's palm with fingers adducted, which is advertised to be 1% TBSA. However, this method can also lead to a 10% to 20% overestimation because the surface areas of the palm with fingers are proportionally smaller, with 0.8% TBSA in men and 0.7% in women.[18]
Proper TBSA calculation will also assist healthcare providers in determining if the patient's burns meet the criteria for transfer to a burn center. Other transfer criteria include burns to the face, genitals, and hands, among other defined criteria by the American Burn Association.[2] Increased volume of burn referrals from single institutions and specific adult ages have not been shown to improve accuracies in determining TBSA.[26]
Other Issues
Human error is inevitable in all aspects of medicine, especially when evaluating burn depth and size. Computer-based smartphone applications are being produced to assist in minimizing errors with overestimating and underestimating TBSA percentages. The applications utilize male and female models of standardized small, average, and obese sizes. This modern technology has revealed the variability in reporting TBSA percentages, with up to 60% overestimation and 70% underestimation of the burned surface area.[2][16] Even though not every technological advance is available at all institutions, mobile applications can be used as triaging tools to assist in decision-making and disposition.[16]
Enhancing Healthcare Team Outcomes
The Rule of Nines is a tool healthcare professionals use to assess the total body surface area involved in burn patients. The healthcare team's initial burn surface area measurement is essential in estimating fluid resuscitation requirements. Patients should have resuscitation started promptly due to the massive fluid losses and transferred to the nearest burn center. However, due to evaluator subjectivity, the measurement of TBSA varies. Thus, frequent healthcare provider education training on calculating TBSA and determining burn depths should be performed by certified and experienced burn providers to ensure that adequate standard of care practices are upheld within the community. Moreover, patient care can be improved by referring facilities and sending pictures of the injuries to the burn attending on call to facilitate proper management and triage. Numerous studies have demonstrated the success and economic benefits of telemedicine.[25]
Media
(Click Image to Enlarge)
(Click Image to Enlarge)
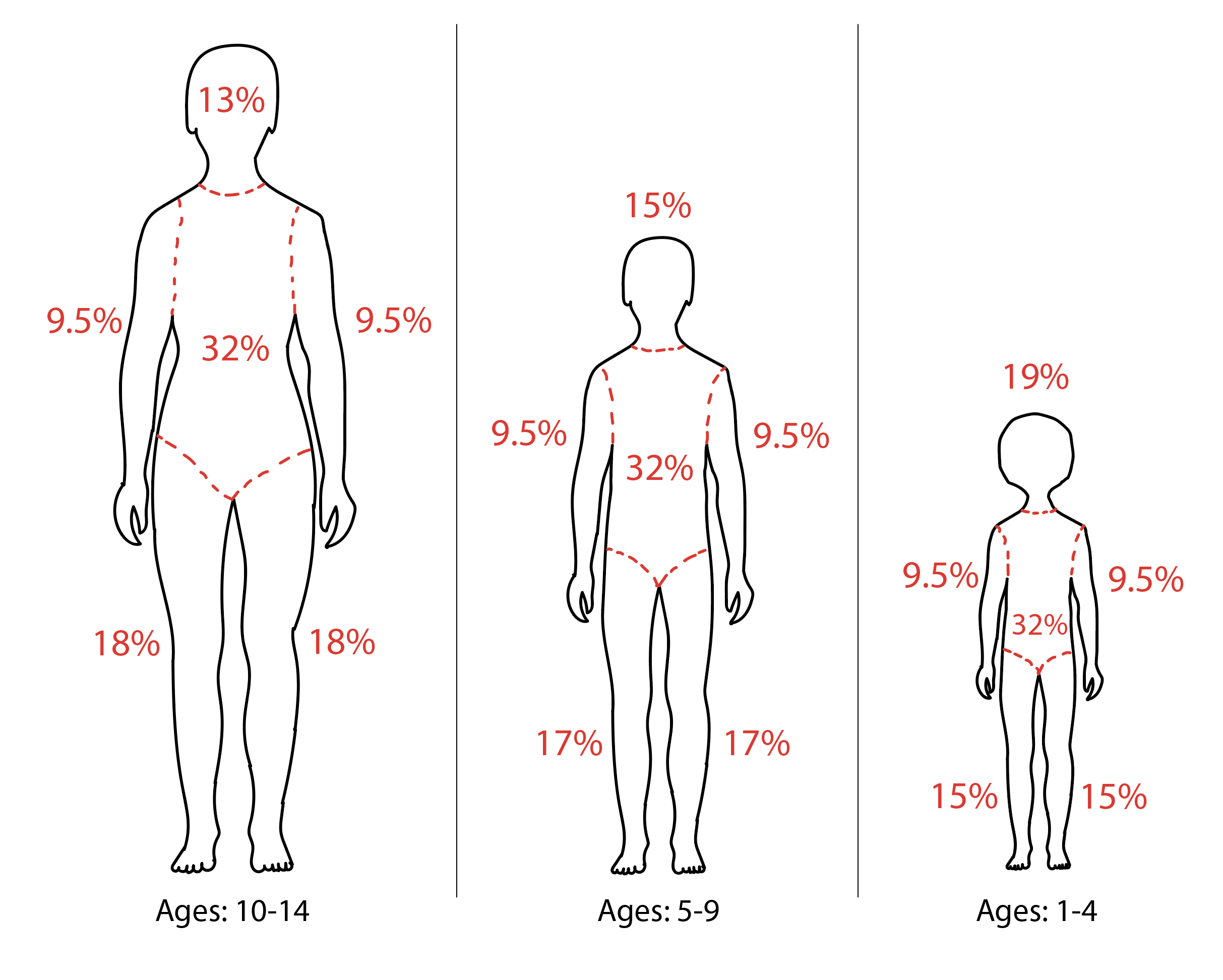
Diagram of Rule of 9s Modifications for Pediatric Patients.
Contributed by Rian Kabir, MD
References
Williams RY, Wohlgemuth SD. Does the "rule of nines" apply to morbidly obese burn victims? Journal of burn care & research : official publication of the American Burn Association. 2013 Jul-Aug:34(4):447-52. doi: 10.1097/BCR.0b013e31827217bd. Epub [PubMed PMID: 23702858]
Level 2 (mid-level) evidenceGiretzlehner M, Ganitzer I, Haller H. Technical and Medical Aspects of Burn Size Assessment and Documentation. Medicina (Kaunas, Lithuania). 2021 Mar 5:57(3):. doi: 10.3390/medicina57030242. Epub 2021 Mar 5 [PubMed PMID: 33807630]
WALLACE AB. The exposure treatment of burns. Lancet (London, England). 1951 Mar 3:1(6653):501-4 [PubMed PMID: 14805109]
Ali SA, Hamiz-Ul-Fawwad S, Al-Ibran E, Ahmed G, Saleem A, Mustafa D, Hussain M. Clinical and demographic features of burn injuries in karachi: a six-year experience at the burns centre, civil hospital, Karachi. Annals of burns and fire disasters. 2016 Mar 31:29(1):4-9 [PubMed PMID: 27857643]
Thom D. Appraising current methods for preclinical calculation of burn size - A pre-hospital perspective. Burns : journal of the International Society for Burn Injuries. 2017 Feb:43(1):127-136. doi: 10.1016/j.burns.2016.07.003. Epub 2016 Aug 27 [PubMed PMID: 27575669]
Level 3 (low-level) evidenceWilliams JF, King BT, Aden JK, Serio-Melvin M, Chung KK, Fenrich CA, Salinas J, Renz EM, Wolf SE, Blackbourne LH, Cancio LC. Comparison of traditional burn wound mapping with a computerized program. Journal of burn care & research : official publication of the American Burn Association. 2013 Jan-Feb:34(1):e29-35. doi: 10.1097/BCR.0b013e3182676e07. Epub [PubMed PMID: 23292593]
Level 1 (high-level) evidenceCheah AKW, Kangkorn T, Tan EH, Loo ML, Chong SJ. The validation study on a three-dimensional burn estimation smart-phone application: accurate, free and fast? Burns & trauma. 2018:6():7. doi: 10.1186/s41038-018-0109-0. Epub 2018 Feb 27 [PubMed PMID: 29497619]
Level 1 (high-level) evidenceTocco-Tussardi I, Presman B, Huss F. Want Correct Percentage of TBSA Burned? Let a Layman Do the Assessment. Journal of burn care & research : official publication of the American Burn Association. 2018 Feb 20:39(2):295-301. doi: 10.1097/BCR.0000000000000613. Epub [PubMed PMID: 28877135]
Borhani-Khomani K, Partoft S, Holmgaard R. Assessment of burn size in obese adults; a literature review. Journal of plastic surgery and hand surgery. 2017 Dec:51(6):375-380. doi: 10.1080/2000656X.2017.1310732. Epub 2017 Apr 18 [PubMed PMID: 28417654]
Rosenthal J, Clark A, Campbell S, McMahon M, Arnoldo B, Wolf SE, Phelan H. Effects of obesity on burn resuscitation. Burns : journal of the International Society for Burn Injuries. 2018 Dec:44(8):1947-1953. doi: 10.1016/j.burns.2018.06.002. Epub 2018 Oct 31 [PubMed PMID: 30391062]
Alvarado R, Chung KK, Cancio LC, Wolf SE. Burn resuscitation. Burns : journal of the International Society for Burn Injuries. 2009 Feb:35(1):4-14. doi: 10.1016/j.burns.2008.03.008. Epub 2008 Jun 9 [PubMed PMID: 18539396]
Greenhalgh DG, Cartotto R, Taylor SL, Fine JR, Lewis GM, Smith DJ Jr, Marano MA, Gibson A, Wibbenmeyer LA, Holmes JH, Rizzo JA, Foster KN, Khandelwal A, Fischer S, Hemmila MR, Hill D, Aballay AM, Tredget EE, Goverman J, Phelan H, Jimenez CJ, Baldea A, Sood R. Burn Resuscitation Practices in North America: Results of the Acute Burn ResUscitation Multicenter Prospective Trial (ABRUPT). Annals of surgery. 2023 Mar 1:277(3):512-519. doi: 10.1097/SLA.0000000000005166. Epub 2021 Aug 19 [PubMed PMID: 34417368]
Romanowski KS, Palmieri TL. Pediatric burn resuscitation: past, present, and future. Burns & trauma. 2017:5():26. doi: 10.1186/s41038-017-0091-y. Epub 2017 Sep 4 [PubMed PMID: 28879205]
Parvizi D, Giretzlehner M, Dirnberger J, Owen R, Haller HL, Schintler MV, Wurzer P, Lumenta DB, Kamolz LP. The use of telemedicine in burn care: development of a mobile system for TBSA documentation and remote assessment. Annals of burns and fire disasters. 2014 Jun 30:27(2):94-100 [PubMed PMID: 26170783]
Vaughn L, Beckel N, Walters P. Severe burn injury, burn shock, and smoke inhalation injury in small animals. Part 2: diagnosis, therapy, complications, and prognosis. Journal of veterinary emergency and critical care (San Antonio, Tex. : 2001). 2012 Apr:22(2):187-200. doi: 10.1111/j.1476-4431.2012.00728.x. Epub [PubMed PMID: 23016810]
Level 3 (low-level) evidenceColson CD, Alberto EC, Milestone ZP, Batra N, Salvador T, Fooladi H, Cleary K, Izem R, Burd RS. EasyTBSA as a method for calculating total body surface area burned: a validation study. Emergency medicine journal : EMJ. 2023 Apr:40(4):279-284. doi: 10.1136/emermed-2022-212308. Epub 2023 Jan 13 [PubMed PMID: 36639224]
Level 1 (high-level) evidencePham C, Collier Z, Gillenwater J. Changing the Way We Think About Burn Size Estimation. Journal of burn care & research : official publication of the American Burn Association. 2019 Jan 1:40(1):1-11. doi: 10.1093/jbcr/iry050. Epub [PubMed PMID: 30247559]
Kamolz LP, Lumenta DB, Parvizi D, Dirnberger J, Owen R, Höller J, Giretzlehner M. Smartphones and burn size estimation: "Rapid Burn Assessor". Annals of burns and fire disasters. 2014 Jun 30:27(2):101-4 [PubMed PMID: 26170784]
Liu NT, Fenrich CA, Serio-Melvin ML, Peterson WC, Cancio LC, Salinas J. The impact of patient weight on burn resuscitation. The journal of trauma and acute care surgery. 2017 Jul:83(1 Suppl 1):S112-S119. doi: 10.1097/TA.0000000000001486. Epub [PubMed PMID: 28452888]
Livingston EH, Lee S. Percentage of burned body surface area determination in obese and nonobese patients. The Journal of surgical research. 2000 Jun 15:91(2):106-10 [PubMed PMID: 10839957]
Stevens JV, Prieto NS, Ridelman E, Klein JD, Shanti CM. Weight-based vs body surface area-based fluid resuscitation predictions in pediatric burn patients. Burns : journal of the International Society for Burn Injuries. 2023 Feb:49(1):120-128. doi: 10.1016/j.burns.2022.03.007. Epub 2022 Mar 19 [PubMed PMID: 35351355]
Pisano C, Fabia R, Shi J, Wheeler K, Giles S, Puett L, Stewart D, Ziegfeld S, Flint J, Miller J, Aguayo P, Alberto EC, Burd RS, Vitale L, Klein J, Thakkar RK. Variation in acute fluid resuscitation among pediatric burn centers. Burns : journal of the International Society for Burn Injuries. 2021 May:47(3):545-550. doi: 10.1016/j.burns.2020.04.013. Epub 2020 May 16 [PubMed PMID: 33707085]
Prieto MF, Acha B, Gómez-Cía T, Fondón I, Serrano C. A system for 3D representation of burns and calculation of burnt skin area. Burns : journal of the International Society for Burn Injuries. 2011 Nov:37(7):1233-40. doi: 10.1016/j.burns.2011.05.018. Epub 2011 Jun 23 [PubMed PMID: 21703768]
Neaman KC, Andres LA, McClure AM, Burton ME, Kemmeter PR, Ford RD. A new method for estimation of involved BSAs for obese and normal-weight patients with burn injury. Journal of burn care & research : official publication of the American Burn Association. 2011 May-Jun:32(3):421-8. doi: 10.1097/BCR.0b013e318217f8c6. Epub [PubMed PMID: 21562463]
Level 2 (mid-level) evidenceTran DP, Arnold DH, Thompson CM, Richmond NJ, Gondek S, Kidd RS. Evaluating Discrepancies in Percent Total Body Surface Area Burn Assessments Between Prehospital Providers and Burn Center Physicians. Journal of burn care & research : official publication of the American Burn Association. 2022 Jan 5:43(1):225-231. doi: 10.1093/jbcr/irab131. Epub [PubMed PMID: 34289051]
Armstrong JR, Willand L, Gonzalez B, Sandhu J, Mosier MJ. Quantitative Analysis of Estimated Burn Size Accuracy for Transfer Patients. Journal of burn care & research : official publication of the American Burn Association. 2017 Jan/Feb:38(1):e30-e35. doi: 10.1097/BCR.0000000000000460. Epub [PubMed PMID: 28009696]