Introduction
Toxic megacolon is a rare but potentially deadly complication of colonic inflammation. Its definition is a nonobstructive dilation of the colon, which can be total or segmental and is usually associated with systemic toxicity.[1][2] It is most commonly associated with inflammatory bowel disease, especially ulcerative colitis, yet any condition that leads to inflammation of the colon can potentially cause toxic megacolon.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Toxic megacolon can be a potential complication of any disease-causing infectious colitis. The common causes include [2][4]:
Inflammatory Causes
-
Ulcerative colitis
-
Crohn disease
Infectious Causes
-
Clostridium difficile
-
Salmonella
-
Shigella
-
Campylobacter colitis
-
Enterohemorrhagic or enteroaggregative Escherichia coli O157 (can lead to hemolytic-uremic syndrome)
-
Cytomegalovirus
-
Entamoeba
Ischemia
Of note, Cytomegalovirus is the leading cause of toxic megacolon in HIV and AIDS patients, especially in those who have disseminated cytomegalovirus.[4] Whereas Entamoeba is the least common cause [2].
Factors that can precipitate toxic megacolon include, but are not limited to [5]:
- Hypokalemia
-
Medications (antimotility agents, opiates, anticholinergics, antidepressants)
-
Barium enema
-
Colonoscopy & bowel preparations
Epidemiology
The incidence of toxic megacolon in the general population is unknown. Toxic megacolon can occur in males and females of all ages. Nevertheless, people at most risk are those with inflammatory bowel disease, especially in the early phase of the disease.[1] Involvement during early disease can be seen more often in Crohn disease before fibrotic colon damage. Once severe fibrosis occurs, the colon cannot dilate.[6][5] However, the incidence in people with inflammatory bowel disease has been a topic of study, and the results are somewhat conflicting; some studies show higher incidence in patients with ulcerative colitis versus Crohn disease (8 to 10% vs. 2.3%), whereas others show higher incidence in Crohn disease (1 to 2.5% vs. 4.4 to 6.3%).[3][2][6]
Clostridium difficile infection can be asymptomatic or can lead to severe disease with toxic megacolon.[7][8][9] Over the past few years, the number of C. difficile colitis related toxic megacolon cases has been increasing. Before 1990 there was an increase from 0.4% to 3%, and after 1990 to 4.3% in proportion to its prevalence.[3][2] Asymptomatic C. difficile infection occurs in about 20% of hospitalized patients, and symptomatic C. difficile infection presents in 1% of hospitalized patients.[5][10][11][12]
Pathophysiology
The pathogenesis of toxic megacolon is not entirely known. Nevertheless, one of the possible mechanisms proposed suggests that mucosal inflammation initiates the process. It releases inflammatory mediators, bacterial products and increases the production of inducible nitric oxide synthase, which in turn increases nitric oxide, and thus causes dilation of the colon. A study showed that patients with toxic megacolon have significantly high levels of inducible nitric oxide synthase in the muscularis propria, which could support this proposed mechanism.[13] Additionally, toxic megacolon leads to inflammation of the smooth muscle of the colon, which causes its paralysis and eventually dilation.[14]
Histopathology
Dilation of the colon, thinning of the colonic wall, and deep ulcers are gross features that toxic megacolon shares with ulcerative colitis and Crohn’s disease. However, the hallmark of toxic megacolon is acute transmural inflammation of the colon with necrosis and granulation tissue, filled with inflammatory cells, such as neutrophils and lymphocytes. The muscle fibers are usually shortened and rounded with collections of eosinophilic cytoplasm.
A key feature that distinguishes toxic megacolon from the neuropathic process is the presence of submucosal and myenteric plexi within the colon.[5]
History and Physical
A thorough history of the patient is critical. Knowing the patient’s medical history ahead of time, HIV/AIDS status, medications, or exposures can help point physicians towards the right diagnosis. It is imperative to review the patient's medication as some (like steroids) can mask the full picture of toxic megacolon, and others can aggravate it (anticholinergics or opioids, for example).[5] Patients presenting with diarrhea and abdominal pain or distension should increase the suspicion index of toxic megacolon.
Patients with a diagnosis of toxic megacolon will look toxic. Those patients are critically ill and usually present with abdominal pain and distention, nausea, vomiting, diarrhea (may or may not be bloody), and altered sensorium. On physical exam, abdominal tenderness and decreased bowel sounds are usually present.[5][11] In a study that focused on patients with C. difficile infection and toxic megacolon, the three most commonly seen complaints were diarrhea, malaise, and abdominal pain/distension.[11]
Comorbidities are frequently seen in those patients, as well. Clinicians can expect to find fluid and electrolyte imbalance, hypotension, anemia, weight loss, uncomplicated diabetes, and renal failure.[15]
Peritonitis symptoms (fever, abdominal pain, tenderness, altered mental status, hypotension) could indicate bowel perforation. Patients who have received steroids may not show this picture as steroids can mask some of those symptoms. Nevertheless, if the patient continues to have a fever for 2 or 3 days while being treated with steroids, the clinician should consider the possibility of a perforated bowel.[2]
Evaluation
The diagnostic basis is the patient’s systemic symptoms and greater than 6 cm dilation of the colon seen on radiographic images.[2] Below are the most commonly used diagnostic criteria for toxic megacolon (by Jalan et al.) [1][2]:
-
Radiographic evidence of the dilation of the colon greater than 6 cm AND:
-
At least three of the following:
- Fever over 38 degrees C
- Heart rate greater than 120 beats/min
- Neutrophilic leukocytosis exceeding 10500/micro/L
- Anemia
-
At least one of the following:
- Dehydration
- Altered sensorium
- Electrolyte disturbances
- Hypotension
Vital Signs and Laboratory
Vital signs and laboratory results will show fever, tachycardia, anemia, and leukocytosis with a left shift. Increase inflammatory markers, such as erythrocyte sedimentation rate, and C-reactive protein, are also commonly seen. Patients who present with severe diarrhea and volume loss can present with hypokalemia and hypoalbuminemia; this generally indicates poor prognosis.[2]
Radiography
Plain abdominal imaging is still the most frequently utilized modality; however, computed tomography (CT) is seeing increasing use, especially because it can provide more reliable information about the severity of the disease. CT is commonly used to assess possible complications of toxic megacolon, which include abscess, perforation, or ascending pylephlebitis.
Key features visible on CT include colonic wall thickening, pericolic stranding, bands of high and low intensity stretching over thickened submucosal folds (accordion sign), and multilayers appearance due to alternating densities of edematous submucosa and hyperemic mucosa (target sign).
An abdominal ultrasound is also an option, but it provides nonspecific findings that might not always help with diagnosis.[16][2]
Colonoscopy
Colonoscopy is not necessary for diagnosis. Therefore, colonoscopy is discouraged due to the high risk of perforation.[2]
Treatment / Management
The treatment focuses on medical management and supportive care to decompress the colon to avoid perforation. The treatment of the underlying cause, correction of any electrolyte disturbances (ex. hypokalemia), symptom management, and prevention of further complications are also important components of a good treatment plan.[15]
Medical Management
Initial treatment involves supportive therapy and medical management. This approach is usually successful in about half of the patients. Patients should obtain admission to the intensive care unit in case of unexpected deterioration. Initially, checking complete blood count, abdominal films, and electrolytes should take place every 12 hours. Once patients improve, images and labs can scale back to once daily. All the medications which can aggravate the megacolon, such as opioids, anticholinergics, etc., should be stopped. Patients should be started on IV fluids to provide adequate hydration.[17] Due to the high risk of perforation, patients are frequently placed on antibiotics, especially if an infectious cause is suspected. The most commonly used antibiotics are metronidazole or vancomycin.[18][19] If cytomegalovirus is the suspected cause, then gancyclovir should be given.[2] Antibiotics of choice for C. difficile are oral vancomycin or oral fidaxomicin. If those are not available, oral metronidazole is an alternative.[7](A1)
Patients with ulcerative colitis should also be given steroids as soon as possible. Generally, the recommendation is hydrocortisone 100 mg over 6 hours (400 mg daily) or methylprednisone 60 mg daily for 5 days. Higher doses did not show significant benefits.[18] Several studies have shown the benefits of using cyclosporine and infliximab in patients with ulcerative colitis. However, those studies did not use patients who presented with toxic megacolon; thus, they are generally not recommended as part of the treatment.[2](B3)
Lastly, patients must be on bowel rest. A nasogastric tube can be inserted to help decompress the stomach, but it will not decompress the colon. As the patient continues to improve, they can gradually start eating to promote gut healing.[2]
Surgical Management
A surgeon should be involved in the patient's care from day 1, in case intervention might be necessary. The current surgical treatment of choice in acute toxic megacolon is subtotal colectomy with ileostomy and either a Hartmann pouch, sigmoidostomy, or rectostomy. Previously there were two additional surgical methods used: total proctocolectomy and the Turnbull method. Turnbull's method was essentially a colon decompression technique that served to prepare a patient for a colectomy. However, studies showed that this method was associated with increased bleeding and high mortality (71%) versus those with subtotal colectomy with ileostomy (8%). Studies conducted with patients treated with total proctocolectomy showed a mortality of 21%.[3][2](B2)
The exact time of surgery in toxic megacolon patients is still unclear. If there is perforation, bleeding, or clinical deterioration of a patient, surgical intervention is unavoidable. Nevertheless, some studies conclude favorable outcomes in patients where surgical intervention is done soon after making the diagnosis of toxic megacolon, whereas other studies show an increase in mortality, especially in patients older than 65.[20] Therefore, surgeons and hospitalists need to work together and assess the patient on a daily basis.[2] This collaboration is essential because colon perforation correlates with a worse prognosis, and it increases mortality by 3 to 5 times.[3][15](B2)
Differential Diagnosis
Differential diagnosis includes [21][2][22]:
- Hirschsprung disease
- Acquired megacolon
- Colonic pseudo-obstruction (Ogilvie syndrome)
- Diffuse gastrointestinal dysmotility
Prognosis
For patients with inflammatory bowel disease, the mortality rates are around 0 to 2%; this is attributable to multiple factors, such as early intervention and better treatment.[23] Colon perforation correlates with a worse prognosis, and it increases mortality by 3 to 5 times.[3][15] However, according to one study, if the patient has surgery earlier, it can decrease the mortality from 22% to 1.2%, whereas other studies show an increase in mortality, especially in patients older than 65.[24][20]
Complications
If toxic megacolon does not receive proper treatment, it has a risk of rupture. Bowel perforation, peritonitis, abscess, and abdominal compartment syndrome are severe complications that warrant immediate surgical intervention.[2]
Deterrence and Patient Education
Although toxic megacolon is a relatively rare disease, patients should receive education about this condition, especially those with inflammatory bowel disease. Since those patients are at an increased risk of developing toxic megacolon, they should understand the precipitating factors as well as potential symptoms. Early diagnosis and treatment can increase the chances of survival.
Enhancing Healthcare Team Outcomes
Toxic megacolon is a medical emergency that demands urgent attention. Failure to recognize the disorder is associated with high mortality and morbidity. Thus, optimal disorder management is best by an interprofessional team. Assistance from a radiologist is vital to make the diagnosis. These patients need ICU care with close monitoring. Nurses should be aware of the potential complications of the disorder and communicate with the surgeon if the patient has signs of peritonitis. Aggressive hydration, replacement of electrolytes, and antibiotics are essential. The pharmacist should check the patient's medication record to ensure that they are on no medications that cause ileus and is on appropriate antibiotics. While most patients do recover with medical therapy, some may require surgery.
The surgical group should be involved early in the process in case initial therapy fails and surgery is unavoidable. High risk of colon perforation and abdominal compartment syndrome are situations where surgery is necessary to avoid further complications.[2] Medical and surgical teams should evaluate patients daily and determine if they would benefit more from surgery than medical management. Surgical and/or gastroenterology specialty-trained nursing staff can assist in the surgery, monitoring the patient (in surgical and non-surgical cases, respectively), and being aware of possible adverse drug effects. They can also check that treatment is trending positively and alert the treating clinician or surgeon of any relapse. Close communication between interprofessional team members is vital if one wants to improve outcomes. Level III
Disclaimer: This research was supported (in whole or part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Media
(Click Image to Enlarge)

Toxic megacolon Contributed by WikiUser:Hellerhoff; (CC BY-SA 3.0 https://creativecommons.org/licenses/by-sa/3.0/deed.en) Image courtesy: https://commons.wikimedia.org/wiki/File:Toxisches_Megacolon_bei_Colitis_ulcerosa.jpg
(Click Image to Enlarge)
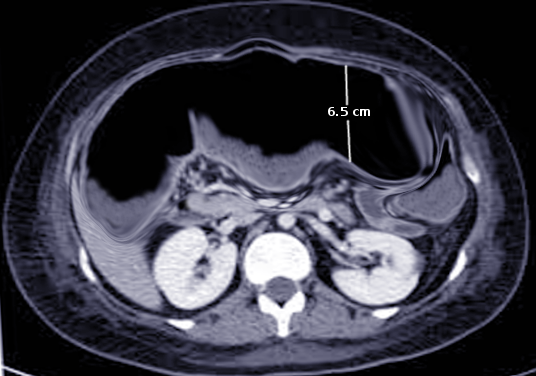
CT Toxic megacolon Image courtesy O.Chaigasame
References
Jalan KN, Sircus W, Card WI, Falconer CW, Bruce CB, Crean GP, McManus JP, Small WP, Smith AN. An experience of ulcerative colitis. I. Toxic dilation in 55 cases. Gastroenterology. 1969 Jul:57(1):68-82 [PubMed PMID: 5305933]
Level 3 (low-level) evidenceAutenrieth DM, Baumgart DC. Toxic megacolon. Inflammatory bowel diseases. 2012 Mar:18(3):584-91. doi: 10.1002/ibd.21847. Epub [PubMed PMID: 22009735]
Ausch C, Madoff RD, Gnant M, Rosen HR, Garcia-Aguilar J, Hölbling N, Herbst F, Buxhofer V, Holzer B, Rothenberger DA, Schiessel R. Aetiology and surgical management of toxic megacolon. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2006 Mar:8(3):195-201 [PubMed PMID: 16466559]
Level 2 (mid-level) evidenceHommes DW,Sterringa G,van Deventer SJ,Tytgat GN,Weel J, The pathogenicity of cytomegalovirus in inflammatory bowel disease: a systematic review and evidence-based recommendations for future research. Inflammatory bowel diseases. 2004 May; [PubMed PMID: 15290919]
Level 1 (high-level) evidenceNorland CC, Kirsner JB. Toxic dilatation of colon (toxic megacolon): etiology, treatment and prognosis in 42 patients. Medicine. 1969 May:48(3):229-50 [PubMed PMID: 5769743]
Grieco MB, Bordan DL, Geiss AC, Beil AR Jr. Toxic megacolon complicating Crohn's colitis. Annals of surgery. 1980 Jan:191(1):75-80 [PubMed PMID: 7352781]
Level 3 (low-level) evidenceMcDonald LC, Gerding DN, Johnson S, Bakken JS, Carroll KC, Coffin SE, Dubberke ER, Garey KW, Gould CV, Kelly C, Loo V, Shaklee Sammons J, Sandora TJ, Wilcox MH. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2018 Mar 19:66(7):e1-e48. doi: 10.1093/cid/cix1085. Epub [PubMed PMID: 29462280]
Level 1 (high-level) evidenceBagdasarian N, Rao K, Malani PN. Diagnosis and treatment of Clostridium difficile in adults: a systematic review. JAMA. 2015 Jan 27:313(4):398-408. doi: 10.1001/jama.2014.17103. Epub [PubMed PMID: 25626036]
Level 1 (high-level) evidenceKelly CP, LaMont JT. Clostridium difficile--more difficult than ever. The New England journal of medicine. 2008 Oct 30:359(18):1932-40. doi: 10.1056/NEJMra0707500. Epub [PubMed PMID: 18971494]
Hokama A, Ohira T, Kishimoto K, Kinjo F, Fujita J. Impending megacolon: small bowel distension as a predictor of toxic megacolon in ulcerative colitis. Internal and emergency medicine. 2012 Oct:7(5):487-8 [PubMed PMID: 22843318]
Level 3 (low-level) evidenceTrudel JL, Deschênes M, Mayrand S, Barkun AN. Toxic megacolon complicating pseudomembranous enterocolitis. Diseases of the colon and rectum. 1995 Oct:38(10):1033-8 [PubMed PMID: 7555415]
Level 2 (mid-level) evidenceBerman L, Carling T, Fitzgerald TN, Bell RL, Duffy AJ, Longo WE, Roberts KE. Defining surgical therapy for pseudomembranous colitis with toxic megacolon. Journal of clinical gastroenterology. 2008 May-Jun:42(5):476-80. doi: 10.1097/MCG.0b013e31804bbe12. Epub [PubMed PMID: 18277885]
Level 3 (low-level) evidenceMourelle M, Casellas F, Guarner F, Salas A, Riveros-Moreno V, Moncada S, Malagelada JR. Induction of nitric oxide synthase in colonic smooth muscle from patients with toxic megacolon. Gastroenterology. 1995 Nov:109(5):1497-502 [PubMed PMID: 7557131]
Level 3 (low-level) evidenceTariq S, Farooq A, Ali I, Wijesinghe H. Toxic colonoscopy--how investigating active inflammatory bowel disease can lead to the serious complication of toxic megacolon. BMJ case reports. 2015 Jul 22:2015():. doi: 10.1136/bcr-2015-209769. Epub 2015 Jul 22 [PubMed PMID: 26202312]
Level 3 (low-level) evidenceDoshi R,Desai J,Shah Y,Decter D,Doshi S, Incidence, features, in-hospital outcomes and predictors of in-hospital mortality associated with toxic megacolon hospitalizations in the United States. Internal and emergency medicine. 2018 Sep; [PubMed PMID: 29948833]
Imbriaco M, Balthazar EJ. Toxic megacolon: role of CT in evaluation and detection of complications. Clinical imaging. 2001 Sep-Oct:25(5):349-54 [PubMed PMID: 11682295]
Level 2 (mid-level) evidencePresent DH, Wolfson D, Gelernt IM, Rubin PH, Bauer J, Chapman ML. Medical decompression of toxic megacolon by "rolling". A new technique of decompression with favorable long-term follow-up. Journal of clinical gastroenterology. 1988 Oct:10(5):485-90 [PubMed PMID: 3183326]
Travis SP, Stange EF, Lémann M, Oresland T, Bemelman WA, Chowers Y, Colombel JF, D'Haens G, Ghosh S, Marteau P, Kruis W, Mortensen NJ, Penninckx F, Gassull M, European Crohn's and Colitis Organisation (ECCO). European evidence-based Consensus on the management of ulcerative colitis: Current management. Journal of Crohn's & colitis. 2008 Mar:2(1):24-62. doi: 10.1016/j.crohns.2007.11.002. Epub 2008 Jan 18 [PubMed PMID: 21172195]
Level 3 (low-level) evidenceHung CW, Wu WF, Wu CL. Rotavirus gastroenteritis complicated with toxic megacolon. Acta paediatrica (Oslo, Norway : 1992). 2009 Nov:98(11):1850-2. doi: 10.1111/j.1651-2227.2009.01444.x. Epub 2009 Jul 24 [PubMed PMID: 19650837]
Level 3 (low-level) evidenceD'Amico C, Vitale A, Angriman I, Ruffolo C, D'Amico F, Valente D, Berto M, Vella V, Scarpa M, D'Amico DF. Early surgery for the treatment of toxic megacolon. Digestion. 2005:72(2-3):146-9 [PubMed PMID: 16172551]
Vanek VW, Al-Salti M. Acute pseudo-obstruction of the colon (Ogilvie's syndrome). An analysis of 400 cases. Diseases of the colon and rectum. 1986 Mar:29(3):203-10 [PubMed PMID: 3753674]
Level 3 (low-level) evidenceDe Giorgio R, Sarnelli G, Corinaldesi R, Stanghellini V. Advances in our understanding of the pathology of chronic intestinal pseudo-obstruction. Gut. 2004 Nov:53(11):1549-52 [PubMed PMID: 15479666]
Level 3 (low-level) evidenceDanovitch SH. Fulminant colitis and toxic megacolon. Gastroenterology clinics of North America. 1989 Mar:18(1):73-82 [PubMed PMID: 2493427]
Flatmark A, Fretheim B, Gjone E. Early colectomy in severe ulcerative colitis. Scandinavian journal of gastroenterology. 1975:10(4):427-31 [PubMed PMID: 1153936]