Introduction
The diagnosis of epicardial coronary artery disease (CAD) during left heart catheterization is made through the angiographic interpretation of percent narrowing of the arterial lumen. The severe stenotic lesions typically have an appearance of at least 70 percent diameter reduction. However, there is often inter-observer variability in the assessment of intermediate lesions (40% to 70% stenosis). These lesions may have functional impairment of flow distally to cause myocardial ischemia and eventually left ventricular contractile dysfunction. The physiologic assessment of such lesions is paramount in the cardiac catheterization lab.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Coronary Anatomy
The purpose of angiography is to visualize the coronary arteries, major branches, or anomalies. Angiography also studies plaque burden, calcification, thrombus, or aneurysms. The major epicardial coronary arteries are left anterior descending (LAD), left circumflex (LCx), and the right coronary artery (RCA). The LAD and LCx arise from the left main coronary artery (LM). The LM and RCA typically originate from the left and right aortic sinus of Valsalva, respectively. The branches of LAD are called diagonals and septals. The branches of the LCx are called obtuse marginals. The RCA usually bifurcates into the right posterior descending artery (RPDA) and right posterolateral artery (RPL). RCA also gives acute marginal branches. These are visualized during an angiogram, and pressure measurement can be performed in these. The cardiac microvasculature is not discreetly visualized during cardiac catheterization.
Physiology
The coronary arteries fill during diastole as the vigorous contraction of the heart during systole allows for little driving pressure. Using the principle of Ohm’s law, V = IR (V is voltage difference, I is current, R is resistance), the coronary pressure and flow are directly related, assuming minimal resistance. The pressure gradient in the coronaries is the difference between a distal coronary bed and aortic root pressure. The pressure gradient could be derived by measuring trans-stenotic gradient at rest or hyperemia, a direct coronary flow reserve (CFR) measurement, or the slope of the relationship between mean gradient and coronary flow. The two most commonly used physiological tools are fractional flow reserve (FFR) and instantaneous wave-free ratio (iFR).
Indications
Functional assessment of a lesion with fractional flow reserve (FFR) or instantaneous wave-free ratio (iFR) is appropriate in case of intermediate stenosis (40% to 70% diameter reduction angiographically), multivessel disease, serial coronary stenoses, nonculprit lesion in acute coronary syndrome, saphenous vein graft disease severity and post-intervention assessment. The various recommendations by major society guidelines are as below:
- The 2014 European Society of Cardiology guidelines recommend the use of FFR to detect a hemodynamically relevant coronary lesion in stable patients when other evidence of ischemia is not available (Class I, Level of Evidence A).[1]
- The 2012 American College of Cardiology/American Heart Association guidelines recommends revascularization of coronary stenoses with FFR ≤ 0.8.[2]
- The 2017 Society of Cardiovascular Angiography and Interventions guidelines recommend that if no stress test is available or if the stress results are indeterminate, the FFR ≤ 0.8 can be used to guide revascularization.[3]
Contraindications
There are no specific contraindications to the measurement of IFR/FFR. Adenosine infusion to measure FFR should be avoided in patients with active bronchial asthma.
Equipment
The miniaturized pressure sensor, which is embedded into a coronary wire is able to carry out pressure measurements with high fidelity. The pressure sensor contains piezo-electric sensors and is made by St. Jude and Philip Volcano. The sensor is typically located at the proximal end of the radiopaque wire tip. The disadvantage of these wires is the potential for signal interference at connecting points. These wires typically have a signal drift of < 7 mmHg/hr. FFR is a ratio of pressure distal to stenosis (Pd) relative to proximal pressure (Pa) during maximal hyperemia or vasodilation [4]. On the other hand, iFR equipment relies on the cardiac mechanics of wave generation. A wave-free period (WFP) exists in diastole, and during this period, the intracoronary pressure and flow decrease in a linear fashion, and the microvascular resistance are minimal. Therefore iFR relies on this WFP to derive coronary pressure assessment without inducing hyperemia.[4]
Personnel
The personnel performing coronary arterial pressure measurements are interventional cardiologists with the assistance of a cardiology fellow or a technician and a nurse.
Preparation
The preparation involves the availability of the equipment and installed software.
Technique or Treatment
After obtaining arterial access via the radial or common femoral artery, the index vessel is engaged with a guiding catheter. The pressure wire product packaging is opened under sterile conditions, flushed with saline, and then zeroed. The wire tip is typically shaped per standard practice based on angulation and tortuosity of the vessel. The wire is then advanced through an introducer and guiding catheter into the coronary artery. Normalization of the waveform is obtained, at the tip of the guide catheter. Pressure wire is then parked, just distal to the stenosis. An iFR measurement is recorded. An iFR ≤ 0.89 may prompt the interventionalist to perform revascularization.
Similarly, during FFR measurement, the pressure wire is placed distal to the stenosis, and a hyperemic agent such as adenosine is administered (15 to 30 mcg bolus in RCA and 20-40 µg bolus in the LM or 140 mcg/kg/min for 3 min via IV infusion). FFR calculation is then obtained. FFR values of less than 0.80 indicate significant stenosis.
Complications
The complications are similar to any PCI and include vessel dissection, perforation, embolism, and coronary spasm. Other complications of a diagnostic catheterization include vascular complications, contrast induced nephropathy, stroke, myocardial infarction, arrhythmias and death.
Clinical Significance
Large randomized controlled trials are now available, which has studied the primary endpoint of all-cause mortality, myocardial infarction (MI), or revascularization in 12 to 24 months in patients treated with iFR/FFR guided PCI. The DEFER trial enrolled 325 patients and showed that patients with FFR values greater than 0.75 did not benefit from percutaneous coronary intervention (PCI); however, patients with FFR less than 0.75 had symptomatic improvement.[5] The FAME trial randomized 1005 patients to either FFR guided PCI or PCI by angiography alone. The primary endpoint of death, MI, or repeat revascularization at 12 months was lower in the FFR guided group and was sustained at 24 months.[6] Similarly, the FAME-2 trial enrolled 1220 patients with a FFR value of ≤0.80 who were randomized to either PCI and optimal medical therapy (OMT) versus OMT alone. The trial was prematurely terminated due to an increased incidence of urgent revascularization in the OMT only group.[7]
The DEFINE-FLAIR and IFR SWEDEHEART trials showed the noninferiority of iFR compared to FFR with the primary outcome of major adverse cardiovascular events at 1 year.[8] A pooled patient-level meta-analysis of these 2 trials revealed that iFR based deferral of revascularization was greater than FFR with similar outcomes in both groups.[9]
Enhancing Healthcare Team Outcomes
After identification of an intermediate severity lesion during angiography, coronary artery pressure measurement with FFR or iFR should be done to determine the use of further intervention, which has shown to improve clinical outcomes.
Nursing, Allied Health, and Interprofessional Team Interventions
Coronary artery pressure measurement is an invasive procedure performed in the cath lab with an interprofessional team approach. While an intervnetional cardiologist perform the procedure with a tech or fellow, the nursing staff assists with continuous monitoring of patients clinical status, delivering medications and handing all equipment.
Nursing, Allied Health, and Interprofessional Team Monitoring
The interprofessional team of nurses, radiation technologists, fellow, and the interventional cardiologist closely monitors vital signs, technical aspects, sterility of the procedure along with the safety of the staff and patient from radiation exposure.
Media
(Click Image to Enlarge)
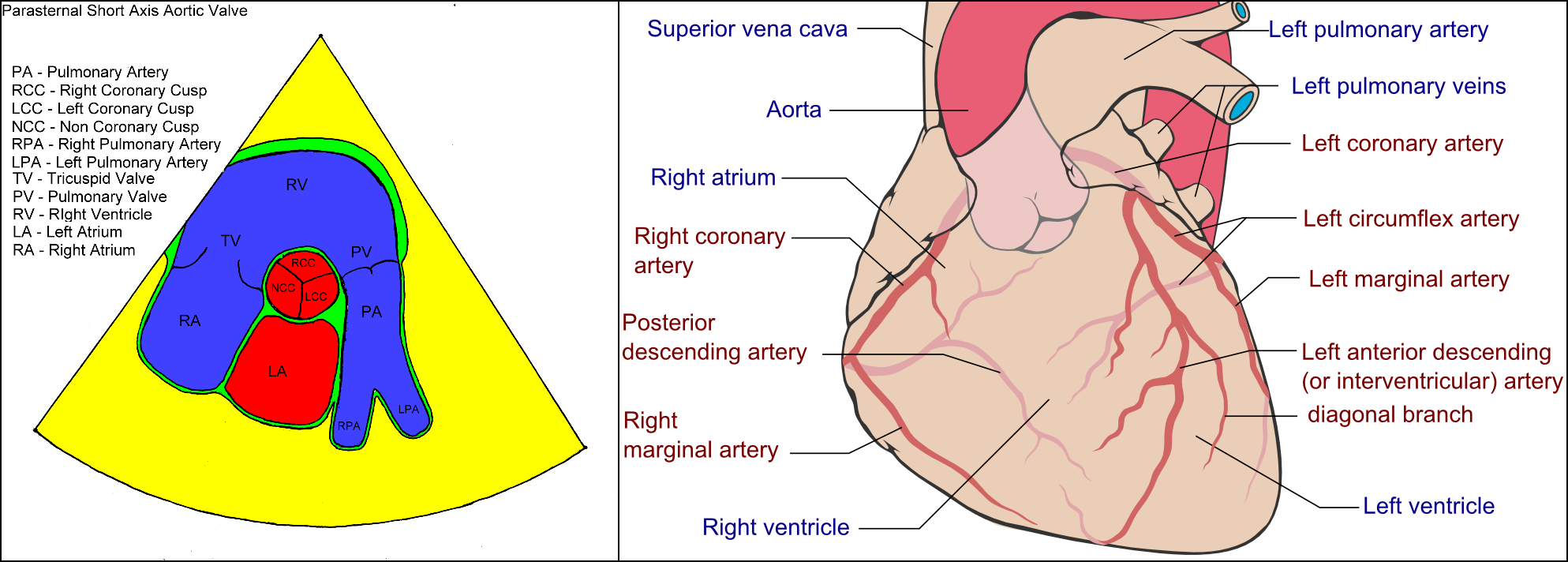
Schematic showing the origination of the coronary arteries. Contributed from Users: Dr Michael Veltman Heart-Scan.org michael.veltman and adaption and further labeling: Mikael Häggström (CC BY-SA 3.0 https://creativecommons.org/licenses/by-sa/3.0/)
References
Kolh P, Windecker S, Alfonso F, Collet JP, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, Jüni P, Kappetein AP, Kastrati A, Knuuti J, Landmesser U, Laufer G, Neumann FJ, Richter DJ, Schauerte P, Sousa Uva M, Stefanini GG, Taggart DP, Torracca L, Valgimigli M, Wijns W, Witkowski A, European Society of Cardiology Committee for Practice Guidelines, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol Ç, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, EACTS Clinical Guidelines Committee, Sousa Uva M, Achenbach S, Pepper J, Anyanwu A, Badimon L, Bauersachs J, Baumbach A, Beygui F, Bonaros N, De Carlo M, Deaton C, Dobrev D, Dunning J, Eeckhout E, Gielen S, Hasdai D, Kirchhof P, Luckraz H, Mahrholdt H, Montalescot G, Paparella D, Rastan AJ, Sanmartin M, Sergeant P, Silber S, Tamargo J, ten Berg J, Thiele H, van Geuns RJ, Wagner HO, Wassmann S, Wendler O, Zamorano JL, Task Force on Myocardial Revascularization of the European Society of Cardiology and the European Association for Cardio-Thoracic Surgery, European Association of Percutaneous Cardiovascular Interventions. 2014 ESC/EACTS Guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2014 Oct:46(4):517-92. doi: 10.1093/ejcts/ezu366. Epub 2014 Aug 29 [PubMed PMID: 25173601]
Fihn SD, Gardin JM, Abrams J, Berra K, Blankenship JC, Dallas AP, Douglas PS, Foody JM, Gerber TC, Hinderliter AL, King SB 3rd, Kligfield PD, Krumholz HM, Kwong RY, Lim MJ, Linderbaum JA, Mack MJ, Munger MA, Prager RL, Sabik JF, Shaw LJ, Sikkema JD, Smith CR Jr, Smith SC Jr, Spertus JA, Williams SV, American College of Cardiology Foundation, American Heart Association Task Force on Practice Guidelines, American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Journal of the American College of Cardiology. 2012 Dec 18:60(24):e44-e164. doi: 10.1016/j.jacc.2012.07.013. Epub 2012 Nov 19 [PubMed PMID: 23182125]
Level 1 (high-level) evidencePatel MR, Calhoon JH, Dehmer GJ, Grantham JA, Maddox TM, Maron DJ, Smith PK. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients With Stable Ischemic Heart Disease : A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. Journal of nuclear cardiology : official publication of the American Society of Nuclear Cardiology. 2017 Oct:24(5):1759-1792. doi: 10.1007/s12350-017-0917-9. Epub [PubMed PMID: 28608183]
Götberg M, Cook CM, Sen S, Nijjer S, Escaned J, Davies JE. The Evolving Future of Instantaneous Wave-Free Ratio and Fractional Flow Reserve. Journal of the American College of Cardiology. 2017 Sep 12:70(11):1379-1402. doi: 10.1016/j.jacc.2017.07.770. Epub [PubMed PMID: 28882237]
Bech GJ, De Bruyne B, Pijls NH, de Muinck ED, Hoorntje JC, Escaned J, Stella PR, Boersma E, Bartunek J, Koolen JJ, Wijns W. Fractional flow reserve to determine the appropriateness of angioplasty in moderate coronary stenosis: a randomized trial. Circulation. 2001 Jun 19:103(24):2928-34 [PubMed PMID: 11413082]
Level 1 (high-level) evidenceTonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van' t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, Ver Lee PN, MacCarthy PA, Fearon WF, FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. The New England journal of medicine. 2009 Jan 15:360(3):213-24. doi: 10.1056/NEJMoa0807611. Epub [PubMed PMID: 19144937]
Level 1 (high-level) evidenceDe Bruyne B, Pijls NH, Kalesan B, Barbato E, Tonino PA, Piroth Z, Jagic N, Möbius-Winkler S, Rioufol G, Witt N, Kala P, MacCarthy P, Engström T, Oldroyd KG, Mavromatis K, Manoharan G, Verlee P, Frobert O, Curzen N, Johnson JB, Jüni P, Fearon WF, FAME 2 Trial Investigators. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. The New England journal of medicine. 2012 Sep 13:367(11):991-1001. doi: 10.1056/NEJMoa1205361. Epub 2012 Aug 27 [PubMed PMID: 22924638]
Level 1 (high-level) evidenceDavies JE, Sen S, Dehbi HM, Al-Lamee R, Petraco R, Nijjer SS, Bhindi R, Lehman SJ, Walters D, Sapontis J, Janssens L, Vrints CJ, Khashaba A, Laine M, Van Belle E, Krackhardt F, Bojara W, Going O, Härle T, Indolfi C, Niccoli G, Ribichini F, Tanaka N, Yokoi H, Takashima H, Kikuta Y, Erglis A, Vinhas H, Canas Silva P, Baptista SB, Alghamdi A, Hellig F, Koo BK, Nam CW, Shin ES, Doh JH, Brugaletta S, Alegria-Barrero E, Meuwissen M, Piek JJ, van Royen N, Sezer M, Di Mario C, Gerber RT, Malik IS, Sharp ASP, Talwar S, Tang K, Samady H, Altman J, Seto AH, Singh J, Jeremias A, Matsuo H, Kharbanda RK, Patel MR, Serruys P, Escaned J. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. The New England journal of medicine. 2017 May 11:376(19):1824-1834. doi: 10.1056/NEJMoa1700445. Epub 2017 Mar 18 [PubMed PMID: 28317458]
Götberg M, Christiansen EH, Gudmundsdottir IJ, Sandhall L, Danielewicz M, Jakobsen L, Olsson SE, Öhagen P, Olsson H, Omerovic E, Calais F, Lindroos P, Maeng M, Tödt T, Venetsanos D, James SK, Kåregren A, Nilsson M, Carlsson J, Hauer D, Jensen J, Karlsson AC, Panayi G, Erlinge D, Fröbert O, iFR-SWEDEHEART Investigators. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. The New England journal of medicine. 2017 May 11:376(19):1813-1823. doi: 10.1056/NEJMoa1616540. Epub 2017 Mar 18 [PubMed PMID: 28317438]