Introduction
The back is a key topographical region of the body, with crucial importance for posture, locomotion, and upper and lower limb movements.[1]
The spine, located in the midline, divides the body into unequal anterior and posterior segments. In the posterior segment, the body area between the neck and gluteal regions is defined as the back region. It lies with the neck superiorly and the pelvis inferiorly.
The back consists of skin and fascia overlying the spine, scapulae, muscle groups, nerves, vessels, and the presacral vertebrae. The primary movements of the back are flexion/extension, lateral bending, and rotation of the trunk. Some of the back muscles attach to the lateral and posterior processes of the vertebrae and help the spine maintain an upright posture, while others are involved in upper extremity movement.[1]
The back muscles are divided into three layers deep, intermediate, and superficial. In some literature, these muscles are also termed extrinsic and intrinsic back muscles (see Image. Extrinsic Back Muscles). This article examines the back muscles in the deep, intermediate, and superficial groups (see Image. Anatomy of the Back Muscles).
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The back is covered by the superficial and deep fascia. The superficial fascia acts as a layer of thickness and strength.[2] It is made up of areolar connective or adipose tissue immediately deep side of the skin of the back. This fascia is continuous with the superficial fascia of the cervical, gluteal, and upper extremities.
The deep fascia of the neck and the back area, a dense fibrous structure, is attached to the occipital bone, spinous processes of the vertebrae, and the iliac crest. The thoracolumbar fascia (TLF), which also may be classified as a strong aponeurosis, is located between the twelfth rib and the iliac crest. The middle fibers of the transversus muscle and upper fibers of the internal oblique muscle lie as the thoracolumbar fascia. Moreover, there are a number of ligaments that lie between the thoracal vertebrae and the parts of the ribs and between successive vertebrae. One of these ligaments, the ligamentum nuchae, is a fibrous membrane. It starts from the external occipital protuberance and attaches to the spinous process of the cervical vertebrae. While in lower animals, it helps to sustain the head position; it is exclusively the rudiment of an important ligament in humans.
The back serves many different functions in the human body. It primarily serves as the primary structural support for the human torso and allows flexibility for movement. Running centrally down the posterior midline is the spinal column.
The spinal column is composed of bony vertebrae, which house and protect the human spinal cord.[1] The column is a continuation of the seven cervical vertebrae in the neck and is composed of twelve thoracic vertebrae, located more superiorly, and five inferior lumbar vertebrae. The column terminates in the sacrum. Ribs articulate with the twelve thoracic vertebrae. Two bony scapulae are situated on either side of the spinal column laterally.[3] They functionally provide a bony attachment for several muscles, including the rotator cuff muscles of the upper extremity.[3]
In addition to the bones, three groups of muscles comprise the back. These muscles are grouped as the intrinsic muscle group, also known as the deep, superficial, and intermediate muscle groups.[4] These groups allow primary movements in the back, including flexion/extension, rotation, side bending, a locomotor function of the limbs, and assistance in the respiratory effort.[4] In addition to supporting respiratory function, these muscles are also involved in supporting the trunk, posture, and locomotor functions of the whole body.
Embryology
The three germ layers in human development are the ectoderm, the mesoderm, and the endoderm.[5] The paraxial mesoderm, which forms the dermis of the skin, also develops the skeletal muscles in the body and the majority of the axial skeleton.[5] The epidermis of the skin in the back derives from the ectoderm.[5] The spinal cord derives from an ectodermal structure called the neural plate.[6][5] The neural plate develops neural folds bilaterally that rise, come together, and fuse to form the neural tube.[6] The tube completely fuses and separates from communication with the amniotic cavity by day 27. Failure of this fusion to occur can result in anencephaly.[7]
The superficial and intermediate muscles of the back are termed "extrinsic" because they originate embryologically from hypaxial myotomes. Intrinsic back muscles develop from epaxial myotomes.[8]
Blood Supply and Lymphatics
Blood supply to the skin and muscles in the back is primarily from the dorsal branches of the posterior intercostal arteries. These arteries arise from intercostal arteries or directly from the descending aorta in some variants.[9] The intercostal arteries run in a groove along with the intercostal vein and nerve caudal to the ribs.[10][11] The thoracic aorta runs anteriorly to the vertebral column and slightly lateral on the left side. The azygos and hemiazygous veins may also be present anterior to the spinal cord. The spinal cord itself has several different sources of blood supply, depending on location and embryological development.[1]
The anterior spinal artery, the posterior spinal arteries, and the artery of Adamkiewicz are responsible for vascular supply to the spinal cord.[1][12] The anterior and posterior intercostal veins are responsible for the venous blood supply of the back.[13][8]
Nerves
Nervous supply to the back primarily arises from dorsal branches of spinal nerves, also known as posterior rami. The sensory innervation to the back organizes in a dermatomal pattern, which corresponds to a specific spinal nerve at different spinal nerves.[14] In addition to providing sensation to the skin of the back, the dorsal branches also serve to innervate the intrinsic muscles of the back.[15] This innervation is in contrast to the extrinsic muscles of the back, which are innervated by spinal nerves.[16]
Muscles
The muscles of the back are divided into three categories (see Image. Surface Anatomy of the Back).[4]
The first category is the superficial back muscles; these are part of the extrinsic back muscle.[3] These muscles are located superficially, and they assist in the movement of the upper limbs.[3] The superficial muscles include:
- Trapezius
- Originates from the superior nuchal line, external occipital protuberance, nuchal ligament, and spinous processes of C7-T12
- Attach to the lateral third of the clavicle, acromion, and spine of the scapula
- Innervated by the accessory nerve (12th cranial nerve)
- Latissimus dorsi
- Originates from spinous processes of T7-L5, sacrum, thoracolumbar fascia, iliac crest, and 10th through 12th rib
- Inserts to the intertubercular groove of the humerus
- Innervated by the thoracodorsal nerve
- Levator scapulae
- Originates from the transverse processes of the first four cervical vertebrae
- Inserts to the superior angle of the scapula
- Innervated by the dorsal scapular nerve
- Rhomboids*
- Minor
- Originated from the nuchal ligament and spinous processes of C7-T1
- Inserts to the superior part of the medial border of the scapula (the line which is located between the superior angle and trigonum scapula
- Innervated by the dorsal scapular nerve
- Major
- Originated from spinous processes of T2-T5
- Inserts to the inferior part of the medial border of the scapula (the line which is located between the inferior angle and trigonum scapula
- Innervated by the dorsal scapular nerve
- Minor
*Rhomboid major and rhomboid minor are part of the deep shoulder girdle muscle group.[17]
The second group of muscles is the intermediate group. It is part of the extrinsic back muscle. These muscles assist in the human respiratory function and are intimately associated with the ribs.[4] This muscle group consists of the following:
- Serratus posterior inferior
- Originated from the ligamentum nuchae and spinous processes of C7-T3 vertebrae
- Inserts to the superior aspect of 2nd through 5th ribs
- Innervated by the anterior rami of the T1-T4 spinal nerves
- Serratus posterior superior
- Originated from the spinous processes of T11-L3 vertebrae
- Inserts to the inferior border of the 9th through 12th ribs
- Innervated by the T9-T12 spinal nerves
The final group of muscles is known as intrinsic or deep back muscles.[4] These muscles are responsible for the motion of the axial skeleton. A deep fascial layer covers the intrinsic muscles. The deep fascia forms a sheath known as the thoracolumbar fascia, which exists in the thoracic and lumbar regions. This fascia extends in the midline from the medial crest of the sacrum to the ligament nuchae and skull. It attaches laterally to the transverse processes and angles of the ribs. It has anterior, middle, and posterior layers. The posterior layer lies between the lumbar and sacral spinous processes laterally over the surface of the erector spinae muscles. The middle layer starts from the lumbar transverse processes and attaches to the iliac crest and the last rib. The anterior layer covers the quadratus lumborum muscle and attaches to the transverse processes of the lumbar vertebrae and the iliac crest.
This group further subdivides into several categories in the back and neck.
The superficial layer consists of the splenius muscles located in the lateral and posterior neck regions.
The main muscle groups in the intrinsic muscles are the erector spinae muscles and the transversospinalis group.[3] The main movements of these muscles are flexion/extension, side bending, and rotation.[4] The erector spinae group, which is the largest group of the intrinsic back muscles, consists of the following:
- Iliocostalis, most laterally located
- Longissimus, the largest part of the group
- Spinalis, most medially located
The functions of this muscle group are to maintain posture, lengthen the spine, and bend the spine to the side. It is the primary extensor of the back when it runs bilaterally.[4] It acts as a lateral flexor and rotator of the spine unilaterally.[4]
The third component of the intrinsic muscles in the human back is the transversospinalis muscles.[4] It is located between the transverse processes and spinous processes of the vertebrae. These muscles lie deep to the erector spinae muscles.[4] The transversospinalis group contains
- Semispinalis is located in the cervical and thoracal regions and has thoracic, cervicis, and capitis muscles.
- The multifidi lie deep to the semispinalis muscles, located along the entire spine, particularly in the lumbar region.
- The rotatores are the deepest part of this group, located along the entire spine, particularly in the thoracic region.
Like the erector spinae group, the transversospinalis group is located bilaterally on the vertebral column. These muscles assist in bending the back posteriorly when contracted bilaterally.[4] When unilateral contraction occurs, they assist with lateral bending and rotation.[4]
Physiologic Variants
It is known that a connection between the latissimus dorsi muscle and the teres major muscle may exist through muscle fibers (with a frequency of 10%) and that the latissimus dorsi muscle may be pierced by the radial nerve or a communicating branch between the radial nerve and the axillary nerve.[18]
The numerical variants of the vertebrae in the thoracolumbar region can be considered a potential risk factor for the clinical symptoms of the back.[19]
Surgical Considerations
The primary surgical considerations with the back must consider the needle placement for administering spinal anesthesia before surgical procedures. The conus medullaris is the most distal end of the spinal cord. It terminates at the level of L2/L3 in newborns and L1 level in adults.[20][21] The surgeon inserts a needle into the dural sac between the L3/L4 levels in adults to avoid the conus medullaris during the administration of anesthesia prior to surgery.[21]
Clinical Significance
Back pain is a common presenting symptom in patients, and in general, conservative treatment, including physical therapy and anti-inflammatory and/or muscle relaxant medications, is enough to mitigate pain. However, the most important thing in this intervention is to reveal the etiology that causes back pain and to treat this cause.[22] Although acute low back pain often resolves on its own, it recurs frequently and becomes chronic low back pain in a substantial group of patients.[23]
Generalized back pain is a common presenting symptom for patients with spinal diseases. The underlying etiology of the pain most commonly is from skeletal muscle strain. It may be caused by herniation of a vertebral disc or spinal disease. The differential for back pain is vast, and lumbar disc issues, including herniation or rupture, and vertebral fractures, all merit consideration.[24] Additionally, osteoarthritis and spondylolisthesis, a condition where a vertebra slips anteriorly compared to the others in the column, can both be causes of back pain.[25] Due to spinal attachment points of the paraspinal muscles, spinal disease studies have focused on these muscle structures in recent years. For this reason, it is becoming increasingly important that the quantity and quality of the paraspinal muscles are important factors leading to spinal cord diseases.[26]
Persistent pain following spine surgery
The terminological approach, which entered the literature in the 1970s as "post-laminectomy syndrome" and "failed back surgery syndrome" (FBSS), was revised as "chronic pain after spinal surgery" (CPSS) in ICD-11 in 2019. This term describes pain that does not subside or even worsens following spine surgery.[27]
Spina bifida
Spina bifida is a congenital condition seen on the back when there is incomplete closure of the vertebral column. There are three different subcategories of the condition.[28]
- Spina bifida occulta results from the incomplete fusion of the vertebral arch. The patients are usually asymptomatic, and the only clinical index of suspicion may be a small tuft of hair overlying the defect.[28]
- Spina bifida cystica with meningocele occurs when the bony vertebral arch fails to form and there is a herniation of the spinal meninges.[28]
- Spina bifida cystica with meningomyelocele is the most severe and involves herniation of the meninges and the spinal cord.[29]
Other Issues
The thoracolumbar fascia (TLF) or lumbodorsal fascia (LF) is an aponeurotic structure prominent in the distal of the thoracic vertebrae, as an undeniable function in an upright posture and load transfer from the upper extremity to the lower extremity.[30][31]
TLF attaches to the spines of the thoracic vertebrae in the midline and closes to the angulus costa of the ribs laterally in the thoracic region, forming a thin cover for the extensor muscles of the vertebral column.[32]
It has three layers in the lumbar region (previously described as just anterior and posterior layers) that surround the erector spine and transversospinalis muscles, which are located between the spinous and transverse processes of the successive vertebra, and the quadratus lumborum muscle, one of the posterior abdominal wall muscles.[31] These three layers continue by merging deep into the internal oblique muscle, forming the aponeurosis of the transversus abdominis muscle.[31][33]
An article published in 2019 stated that only the inner layer of TLF contains elastic fibers. Still, these fibers in the structure of TLF are insufficient to qualify the entire fascia as "flexible."[34] Recent studies in the literature suggest that the lumbodorsal fascia represents a possible source of idiopathic low back pain because it contains nociceptive-free nerve endings.[35][33]
The triangle of auscultation is located on the upper half of the back region. It is bordered by the trapezius, latissimus dorsi, and the medial margin of the scapula. The floor of the triangle of auscultation contains endothoracic fascia and pleura.[36] For this reason, pulmonary auscultation can be performed on the triangle of auscultation. Intervention to the back through the auscultation triangle can be preferable due to decreased morbidity compared to conventional thoracotomy.[37]
Media
(Click Image to Enlarge)
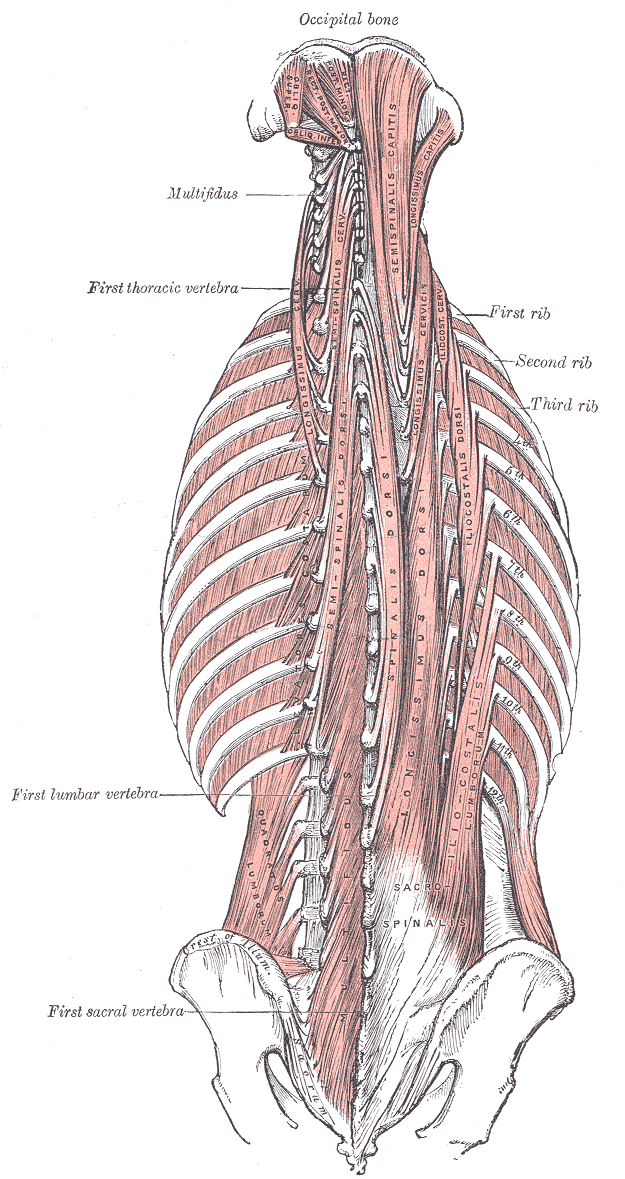
Anatomy of the Back Muscles. The diagram includes the major and minor oblique muscles of the head, occipital bone, oblique superior and inferior, rectus posterior major and minor, semispinalis capitis, longissimus capitis, semispinalis cervicis, longissimus cervicis, semispinalis dorsi, spinalis dorsi, longissimus dorsi, iliocostalis dorsi, iliocostalis lumborum, multifidus, quadratus lumborum, sacrospinalis, and crest of the ilium.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
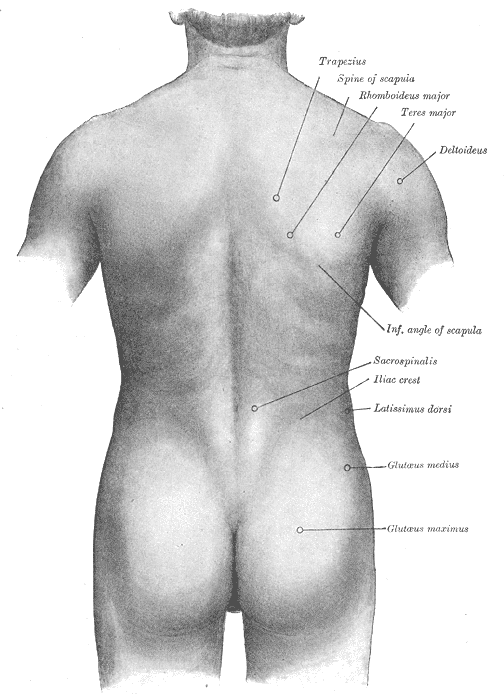
Surface Anatomy of the Back. This illustration shows the trapezius, spine of the scapula, rhomboideus major, teres major, deltoideus, inferior angle of the scapula, sacrospinalis, iliac crest, latissimus dorsi, and glutaeus medius and maximus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
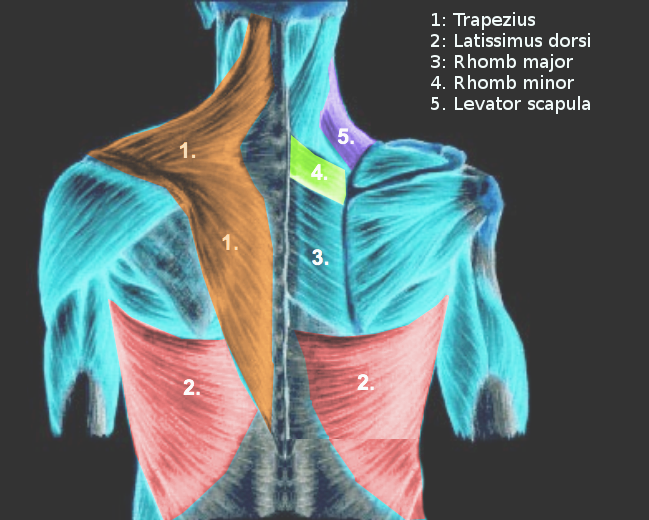
Extrinsic Back Muscles. Shown in this illustration are the trapezius, latissimus dorsi, rhomboid major and minor, and levator scapulae.
Contributed by S Bhimji, MD
References
Kaiser JT, Reddy V, Lugo-Pico JG. Anatomy, Back, Spinal Cord Arteries. StatPearls. 2024 Jan:(): [PubMed PMID: 30725904]
Waxenbaum JA, Woo MJ, Lu M. Physiology, Muscle Energy. StatPearls. 2024 Jan:(): [PubMed PMID: 32644455]
Mitchell B, Imonugo O, Tripp JE. Anatomy, Back, Extrinsic Muscles. StatPearls. 2024 Jan:(): [PubMed PMID: 30725901]
Henson B,Edens MA, Anatomy, Back, Muscles 2018 Jan; [PubMed PMID: 30725759]
Kiecker C, Bates T, Bell E. Molecular specification of germ layers in vertebrate embryos. Cellular and molecular life sciences : CMLS. 2016 Mar:73(5):923-47. doi: 10.1007/s00018-015-2092-y. Epub 2015 Dec 14 [PubMed PMID: 26667903]
Hall BK. Germ layers, the neural crest and emergent organization in development and evolution. Genesis (New York, N.Y. : 2000). 2018 Jun:56(6-7):e23103. doi: 10.1002/dvg.23103. Epub 2018 Apr 10 [PubMed PMID: 29637683]
Gole RA, Meshram PM, Hattangdi SS. Anencephaly and its associated malformations. Journal of clinical and diagnostic research : JCDR. 2014 Sep:8(9):AC07-9. doi: 10.7860/JCDR/2014/10402.4885. Epub 2014 Sep 20 [PubMed PMID: 25386414]
Sato T, Koizumi M, Kim JH, Kim JH, Wang BJ, Murakami G, Cho BH. Fetal development of deep back muscles in the human thoracic region with a focus on transversospinalis muscles and the medial branch of the spinal nerve posterior ramus. Journal of anatomy. 2011 Dec:219(6):756-65. doi: 10.1111/j.1469-7580.2011.01430.x. Epub 2011 Sep 29 [PubMed PMID: 21954879]
Kocbek L, Rakuša M. Common trunk of the posterior intercostal arteries from the thoracic aorta: anatomical variation, frequency, and importance in individuals. Surgical and radiologic anatomy : SRA. 2018 Apr:40(4):465-470. doi: 10.1007/s00276-018-2000-x. Epub 2018 Mar 12 [PubMed PMID: 29532168]
Dewhurst C, O'Neill S, O'Regan K, Maher M. Demonstration of the course of the posterior intercostal artery on CT angiography: relevance to interventional radiology procedures in the chest. Diagnostic and interventional radiology (Ankara, Turkey). 2012 Mar-Apr:18(2):221-4. doi: 10.4261/1305-3825.DIR.4366-11.1. Epub 2011 Nov 28 [PubMed PMID: 22125216]
Level 2 (mid-level) evidenceChoi S,Trieu J,Ridley L, Radiological review of intercostal artery: Anatomical considerations when performing procedures via intercostal space. Journal of medical imaging and radiation oncology. 2010 Aug; [PubMed PMID: 20718909]
Bley TA,Duffek CC,François CJ,Schiebler ML,Acher CW,Mell M,Grist TM,Reeder SB, Presurgical localization of the artery of Adamkiewicz with time-resolved 3.0-T MR angiography. Radiology. 2010 Jun [PubMed PMID: 20501724]
Level 2 (mid-level) evidenceGailloud P, Spinal Vascular Anatomy. Neuroimaging clinics of North America. 2019 Nov [PubMed PMID: 31677734]
Whitman PA, Launico MV, Adigun OO. Anatomy, Skin, Dermatomes. StatPearls. 2024 Jan:(): [PubMed PMID: 30571022]
Bogduk N,Wilson AS,Tynan W, The human lumbar dorsal rami. Journal of anatomy. 1982 Mar; [PubMed PMID: 7076562]
Bayot ML, Nassereddin A, Varacallo M. Anatomy, Shoulder and Upper Limb, Brachial Plexus. StatPearls. 2024 Jan:(): [PubMed PMID: 29763192]
Farrell C, Kiel J. Anatomy, Back, Rhomboid Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30521277]
Ranade AV, Rai R, Rai AR, Dass PM, Pai MM, Vadgaonkar R. Variants of latissimus dorsi with a perspective on tendon transfer surgery: an anatomic study. Journal of shoulder and elbow surgery. 2018 Jan:27(1):167-171. doi: 10.1016/j.jse.2017.06.046. Epub 2017 Sep 19 [PubMed PMID: 28939333]
Level 3 (low-level) evidenceSugiura K,Morimoto M,Higashino K,Takeuchi M,Manabe A,Takao S,Maeda T,Sairyo K, Transitional vertebrae and numerical variants of the spine : prevalence and relationship to low back pain or degenerative spondylolisthesis. The bone & joint journal. 2021 Jul [PubMed PMID: 34192932]
Asil K, Yaldiz M. Conus Medullaris Levels on Ultrasonography in Term Newborns : Normal Levels and Dermatological Findings. Journal of Korean Neurosurgical Society. 2018 Nov:61(6):731-736. doi: 10.3340/jkns.2016.1212.001. Epub 2018 Oct 30 [PubMed PMID: 30396246]
Rider LS, Marra EM. Cauda Equina and Conus Medullaris Syndromes. StatPearls. 2024 Jan:(): [PubMed PMID: 30725885]
Knezevic NN,Candido KD,Vlaeyen JWS,Van Zundert J,Cohen SP, Low back pain. Lancet (London, England). 2021 Jul 3; [PubMed PMID: 34115979]
Evans L,O [PubMed PMID: 36502448]
Robinson WA, Nassr AN, Sebastian AS. Thoracic disc herniation, avoidance, and management of the surgical complications. International orthopaedics. 2019 Apr:43(4):817-823. doi: 10.1007/s00264-018-04282-x. Epub 2019 Jan 21 [PubMed PMID: 30666348]
Hsieh PC, Lee ST, Chen JF. Lower thoracic degenerative spondylithesis with concomitant lumbar spondylosis. Clinical neurology and neurosurgery. 2014 Mar:118():21-5. doi: 10.1016/j.clineuro.2013.11.019. Epub 2013 Dec 6 [PubMed PMID: 24529224]
Level 2 (mid-level) evidenceGong Z,Li D,Zou F,Liu S,Wang H,Ma X, Low lumbar multifidus muscle status and bone mineral density are important risk factors for adjacent segment disease after lumbar fusion: a case-control study. Journal of orthopaedic surgery and research. 2022 Nov 16; [PubMed PMID: 36384537]
Level 2 (mid-level) evidencePetersen EA, Schatman ME, Sayed D, Deer T. Persistent Spinal Pain Syndrome: New Terminology for a New Era. Journal of pain research. 2021:14():1627-1630. doi: 10.2147/JPR.S320923. Epub 2021 Jun 8 [PubMed PMID: 34135626]
Mühl-Benninghaus R, [Spina bifida]. Der Radiologe. 2018 Jul; [PubMed PMID: 29797041]
Sahni M, Alsaleem M, Ohri A. Meningomyelocele. StatPearls. 2024 Jan:(): [PubMed PMID: 30725644]
Uçar İ,Karartı C,Cüce İ,Veziroğlu E,Özüdoğru A,Koçak FA,Dadalı Y, The relationship between muscle size, obesity, body fat ratio, pain and disability in individuals with and without nonspecific low back pain. Clinical anatomy (New York, N.Y.). 2021 Nov; [PubMed PMID: 34378252]
Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: anatomy, function and clinical considerations. Journal of anatomy. 2012 Dec:221(6):507-36. doi: 10.1111/j.1469-7580.2012.01511.x. Epub 2012 May 27 [PubMed PMID: 22630613]
Abe H,Hayashi S,Kim JH,Murakami G,Rodríguez-Vázquez JF,Jin ZW, Fetal development of the thoracolumbar fascia with special reference to the fascial connection with the transversus abdominis, latissimus dorsi, and serratus posterior inferior muscles. Surgical and radiologic anatomy : SRA. 2021 Jun [PubMed PMID: 33438110]
Sinhorim L, Amorim MDS, Ortiz ME, Bittencourt EB, Bianco G, da Silva FC, Horewicz VV, Schleip R, Reed WR, Mazzardo-Martins L, Martins DF. Potential Nociceptive Role of the Thoracolumbar Fascia: A Scope Review Involving In Vivo and Ex Vivo Studies. Journal of clinical medicine. 2021 Sep 24:10(19):. doi: 10.3390/jcm10194342. Epub 2021 Sep 24 [PubMed PMID: 34640360]
Mense S. Innervation of the thoracolumbar fascia. European journal of translational myology. 2019 Aug 2:29(3):8297. doi: 10.4081/ejtm.2019.8297. Epub 2019 Sep 6 [PubMed PMID: 31579474]
Wilke J, Schleip R, Klingler W, Stecco C. The Lumbodorsal Fascia as a Potential Source of Low Back Pain: A Narrative Review. BioMed research international. 2017:2017():5349620. doi: 10.1155/2017/5349620. Epub 2017 May 11 [PubMed PMID: 28584816]
Level 3 (low-level) evidenceMalik N,Tedder BL,Zemaitis MR, Anatomy, Thorax, Triangle of Auscultation StatPearls. 2022 Jan; [PubMed PMID: 30969656]
Prakash S, Kalra P, Khan Y, Dhal A. Ventral scapular osteochondroma excision through 'triangle of auscultation': A case series. Journal of orthopaedic surgery (Hong Kong). 2020 Jan-Apr:28(1):2309499019892848. doi: 10.1177/2309499019892848. Epub [PubMed PMID: 31916491]
Level 2 (mid-level) evidence