Introduction
To be proficient at airway management, clinicians must thoroughly understand the critical anatomical, physiological, and pathological aspects of the airway. Familiarity with the various tools and techniques designed for airway management is crucial. Knowing the indications, contraindications, and complications of endotracheal intubation is important. Understanding how to confirm the proper placement of an endotracheal tube (ETT) remains essential. Recognizing the differences between adult, pediatric, and neonatal airways and mastering strategies for managing difficult airways are key components of safe and effective airway control.[1]
When managing the airway as part of Advanced Cardiovascular Life Support, the following questions should be considered:
- Is the airway patent?
- Is the advanced airway indicated?
- Is the proper placement of the airway device confirmed?
- Is the tube secure, and is its placement confirmed regularly?
Addressing these questions can guide clinicians in making critical decisions for safe and efficient respiratory support.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The adult airway is narrowest at the glottis, whereas the pediatric airway is narrowest at the subglottis and is located more cephalad and anteriorly. Children aged 12 or younger have a smaller cricothyroid membrane, and their larynx is more compliant, funnel-shaped, and positioned more rostrally. The larger occiput, combined with a shorter neck, makes laryngoscopy more difficult and creates obstacles for aligning the oral, laryngeal, and tracheal axes (see Image. Infant Airway). Achieving a neutral neck position and opening the airway often requires a folded towel or shoulder roll. Proper positioning of the airway is essential for successful intubation, making it important to recognize the differences between the adult and pediatric airways.
The dimensions of the trachea depend on the age and sex of the child (see Image. Tracheal Dimensions to the 20th Birthday).[2] The different formulas that may be used to determine the appropriate size of the ETT are as follows:
- Cole formula (for uncuffed tubes): Internal diameter in millimeters = (age in years)/4 + 4 (F)
- Motoyama formula (for cuffed ETTs in children aged 2 or older): Internal diameter in millimeters = (age in years)/4 + 3.5 (EK)
- Khine formula (for cuffed ETTs in children younger than 2): Internal diameter in millimeters = (age in years)/4 + 3.0
For children aged 1 month to 6 years, ultrasound measurement of the subglottic airway diameter more accurately predicts the appropriately sized ETT compared to traditional formulas based on age and height. However, this method may not be practical in urgent or emergent situations. Therefore, familiarity with the aforementioned airway sizing algorithms is paramount.[3] Cuffed ETTs are preferred to reduce air leaks and pressure necrosis in ventilated patients, as the incidence of laryngospasm may be higher with uncuffed tubes during prolonged intubation. These advantages must be balanced against the larger diameter of the cuffed tube, which may provoke laryngospasm during intubation. Video-assisted laryngoscopy is a newer tool in airway management that enhances visualization of the airway.[4]
Indications
Indications for endotracheal intubation include respiratory failure, either hypoxic or hypercapnic; apnea; reduced level of consciousness, occasionally defined as a Glasgow Coma Scale score of 8 or less; rapid changes in mental status; airway injury or impending airway compromise; high aspiration risk; and laryngeal trauma, which includes all penetrating injuries to the neck, abdomen, and chest.[5][6]
Contraindications
Contraindications to endotracheal intubation include severe airway trauma or obstruction that prevents the safe placement of an ETT. A surgical airway is indicated if an ETT cannot be placed in cases where an airway needs to be secured. A cricothyrotomy or needle cricothyrotomy is an emergent option in adults, which should be converted to a formal tracheostomy as soon as an airway is established. An emergent tracheostomy, sometimes termed a slash tracheostomy, is also an acceptable option.
Cricothyrotomy is rarely performed in pediatric patients who cannot be intubated with an ETT, as an emergent tracheostomy is the preferred approach. The only absolute contraindication to surgical cricothyrotomy is the child's age. The exact age at which a surgical cricothyrotomy can be safely performed is controversial and not well defined, often depending more on the patient's size and body habitus than a specific age. Various sources set the lower age limit for pediatric airway management anywhere from 5 to 12 years. However, according to the Pediatric Advanced Life Support guidelines, the pediatric airway is defined for children aged 1 to 8. Needle cricothyrotomy with transtracheal ventilation should be performed in pediatric patients instead of an incision-based surgical cricothyrotomy, which should then be converted to a formal tracheostomy.
Equipment
Airway Position and Clearance
Upper airway obstruction may be relieved by head tilt, chin lift, or jaw thrust. In infants and children, simple suctioning can help clear the airway using a bulb syringe or any mechanical suction device to remove mucus or other debris. When using a bulb syringe to suction an infant, the mouth must be suctioned before the nose to avoid aspiration. The process involves depressing the bulb syringe, inserting it into the mouth, and then suctioning the nose. Infants are particularly susceptible to vagal stimulation during suctioning, which can lead to bradycardia. Consequently, suctioning should not last more than 10 seconds.
Adjuvants to Upper Airway Obstruction
Adjuvants for relieving upper airway obstruction include the oropharyngeal and nasopharyngeal airways. Oropharyngeal airways should not be used in patients with a severe gag reflex or oral trauma, as they could trigger the gag reflex and lead to aspiration of gastric contents. Various sizes of oral appliances are available. These appliances are measured and sized from the lip to the angle of the jaw. Oropharyngeal airways are useful for patients with spontaneous respirations who need assistance in keeping their airways open, such as those with sleep apnea.
A nasopharyngeal airway is used in patients with an intact gag reflex, trismus, and oral trauma or those who have undergone oral or oropharyngeal surgery, where the oral cavity should not be instrumented. The important factor in sizing a nasopharyngeal airway is not only the tube's width, which may be determined by nostril aperture diameter or the position of the nasal septum and turbinates, but also the patient's stature. The average male adult needs a size 7 port, whereas the average female adult requires a size 6 port. A tall male individual requires a size 8, and a tall female individual requires a size 7, as the patient's vertical height roughly corresponds to the anteroposterior length of the midface and, therefore, the nasal cavity.[7] A study involving 413 infants younger than 12 months found an association between subject height and the nares-vocal cord distance. To place the nasopharyngeal airway in infants, the insertion length should be slightly less than the anthropometric measurement of the nose tip to the earlobe distance.[8]
Bag-Mask Ventilation
Proper bag-mask ventilation is a fundamental maneuver in airway management. Both one- and two-hand techniques are used in adults and children. The one-hand technique is typically effective for neonatal airway management, as a single hand can perform all necessary maneuvers. During simple mask ventilation, upper airway obstruction may be relieved with head tilt, chin lift, jaw thrust, and continuous positive airway pressure. Bag-mask ventilation is also appropriate when preparing for intubation.
Advanced Airway
Advanced airways include supraglottic devices and the ETT. Supraglottic devices include the laryngeal mask airway, laryngeal tube, and esophageal-tracheal device.
A relatively recent advancement in airway management is the development of supraglottic airways, with several devices available. Two popular supraglottic devices, the classic and Pro-Seal laryngeal mask airways, have strong safety and efficacy data in the pediatric population. A manometer is recommended to gauge the inflation pressure of the laryngeal mask airway cuff.
Children with a recent upper respiratory infection are at a higher risk of respiratory complications when using a laryngeal mask airway compared to healthy children. Supraglottic devices, such as the King tube, are often preferred over ETTs in the prehospital setting due to their ease of use and the speed with which they can be deployed. Therefore, a secure airway is rapidly established, particularly in emergent situations where emergency medical technicians or other personnel with less experience in managing pediatric airways are involved.
Esophageal-Tracheal Tube and Endotracheal Intubation
This supraglottic airway device, now commonly used by many emergency medical personnel, is intended for intubating the esophagus. The design of this device enables ventilation through a two-cuffed system and a ported tube. These devices are favored for their ease of use and are available in various sizes, although their application is not commonly extended to pediatric airway management.
Oxygen
Oxygen is a critical component of airway management. Preoxygenation using a nasal cannula, bivalve mask, high-flow oxygen, or bilevel-positive airway pressure (BiPAP) can deliver essential oxygen before intubation.
Bougie
A bougie is a long, semirigid plastic device, also known as a plastic stylet, that is considered an adjunct or rescue device in difficult intubations or part of the primary intubation protocols. This tool serves as a guide to facilitate ETT placement, particularly in scenarios where visualization of the vocal cords is challenging.
Personnel
Ideally, at least 2 additional staff members should be available to assist the primary physician in performing the intubation. These staff members can help administer medications and bag and monitor the patient. The team should include a physician, respiratory therapist, nurse, nursing technician, paramedic, and advanced practice provider.
Preparation
After preoxygenation with cricoid pressure and in-line cervical stabilization, rapid-sequence induction followed by direct laryngoscopy provides the safest and most effective approach for airway preparation. The 4 Ds of a difficult airway are as follows:
- Distortion
- Disproportion
- Dysmobility
- Dentition
The vallecula is a crucial anatomical landmark for healthcare professionals performing intubation. Identifying this structure is essential during oral intubation of the trachea. Either the Macintosh or Miller blade may be used to visualize the posterior pharynx. When using a curved Macintosh laryngoscope, the blade is advanced over the tongue toward the vallecula, where it is positioned and depressed to visualize the glottis and vocal cords. This step enables proper ETT placement. Failure to visualize the vallecula increases the risk of esophageal intubation.
When using the straight-bladed Miller laryngoscope, the blade is advanced past the vallecula and positioned directly over the epiglottis to visualize the vocal cords for ETT placement. The ETT should only be introduced after confirming visualization of the glottis and vocal cords.
An alternative to direct laryngoscopy is video laryngoscopy, using a camera attached to a curved blade. This device is positioned near the vallecular space to visualize the vocal cords and facilitate ETT placement. If no laryngeal structures are visible on the initial attempt, the blade should be withdrawn slowly until the larynx or epiglottis comes into view. This step allows for reassessment of the clinician's position.
Required Equipment and Medications
The required equipment includes the following:
- Laryngoscope
- Carbon dioxide detectors
- Continuous waveform capnography
- Material to fix the tube in place
- Chest x-ray
The following are the dosages of rapid-sequence induction medications:
- Sedatives used for induction
- Etomidate: 0.3 to 0.4 mg/kg
- Fentanyl: 2 to 10 mcg/kg
- Midazolam: 0.1 to 0.3 mg/kg
- Propofol: 1 to 2.5 mg/kg
- Thiopental 3 to 5 mg/kg
- Paralytic agents
- Succinylcholine: 1 to 2 mg/kg
- Rocuronium 0.6 to 1.2 mg/kg
- Vecuronium 0.15 to 0.25 mg/kg
Technique or Treatment
The intubation technique involves the following steps:
- Preoxygenation
- Administration of rapid-sequence induction medications
- Application of cricoid pressure
- In-line cervical stabilization followed by laryngoscopy (direct or indirect)
This technique is considered the safest and most effective approach to securing the airway.
The gold standard for assessing ETT placement involves direct visualization using a laryngoscope. Additional methods for confirming proper ETT placement include end-tidal carbon dioxide measurement, capnography waveform analysis, chest x-ray, ultrasound, and clinical assessment. The American Heart Association recommends continuous waveform capnography alongside clinical assessment as the most reliable method for confirming and monitoring correct ETT placement. Bedside mobile ultrasound is another resource available in some emergency departments, whereas many clinicians frequently use chest x-rays. The ideal ETT position is 2 cm above the carina.
Complications of intubation may include esophageal intubation or right mainstem bronchus intubation. Blind intubation often results in the tube entering the right mainstem bronchus. Repositioning may be required if abnormal placement is observed on an x-ray or identified by a flat capnography waveform and a documented value of 0 mm Hg, as the normal range for proper placement is 35 to 45 mm Hg. Clinically, abnormal ETT placement may be detected by finding absent breath sounds on the left chest during auscultation in cases of right mainstem intubation or bilaterally absent breath sounds in esophageal intubation. With esophageal intubation, air may be auscultated over the midepigastric region during ventilation, and oxygen saturation levels drop.
Once the ETT position is confirmed, it must be secured to prevent dislodgement. Then, continuous monitoring with waveform capnography and pulse oximetry is performed. Pediatric intensive care specialists prefer to use a cuffed ETT instead of an uncuffed ETT to prevent air leaks.
Airway Management in Trauma Patients
Trauma is a leading cause of morbidity and mortality worldwide, particularly among individuals aged 15 to 50. Trauma is the second most common single cause of death, representing 8% of all mortalities. The World Health Organization estimates that traumatic injuries from traffic accidents, drowning, poisoning, falls, burns, and violence result in over 5 million deaths worldwide annually, with millions more suffering from the consequences of injuries.
Rapid evacuation and transportation to a trauma center significantly improve the outcome of severely injured patients. However, prehospital intubation is controversial in the Emergency Medical Services (EMS) literature. The medical director of an EMS service typically dictates the clinical context in which paramedics are allowed to intubate in the field. The EMS monitors and transports these patients quickly and safely to the nearest trauma facility.
Surgical Airway
The only absolute contraindication to surgical cricothyroidotomy is the child's age. However, the specific age at which surgical cricothyroidotomy becomes safe remains controversial and lacks a precise definition. Various sources suggest lower age limits between 5 and 12 years. Meanwhile, Pediatric Advanced Life Support defines the pediatric airway as applying to children aged 1 to 8.
Complications
Complications from intubation may include the inability to secure the airway, esophageal intubation, and respiratory failure, either hypoxic or hypercapnic, which can lead to arrest. Other risks include injury to the oropharyngeal or laryngeal airway, resulting in bleeding, soft tissue swelling, and vocal cord damage.
Notably, potential complications such as tension pneumothorax and air leaks from bronchial injuries can arise when intubating patients with chest injuries. Patients with pneumothorax should receive a chest tube before intubation. In cases of bronchial injury, intubation can trigger a significant air leak. In such situations, a bronchial blocker may be used to occlude the damaged lung segment, preventing further air escape.
Clinical Significance
Key considerations in airway management include:
- Differences between pediatric and adult airways
- Selection of the appropriate airway management approach
- Indications, techniques, and medications used in rapid-sequence induction
- Assessment of a difficult airway
- Alternate techniques to achieve a definitive airway
- Various adjuvants in airway management
- Airway management in special circumstances, such as penetrating trauma
- Importance of training and practice in pediatric airway management for prehospital personnel
- Indications, contraindications, and complications of endotracheal intubation
- Confirmation of successful EET placement
Enhancing Healthcare Team Outcomes
An interprofessional team approach involving clinicians; midlevel practitioners, such as physician assistants and nurse practitioners; and emergency medical staff—supported by good preparation, preoxygenation, and the recognition of difficult airways—significantly enhances the success of airway management. Adjusting the plan when difficulty is anticipated is both prudent and safe, reducing failed intubation rates and improving patient outcomes.
All personnel involved should regularly sharpen their skills, either in the field or in a simulation laboratory. Proper training significantly improves intubation success rates and reduces mortality than the specific field of medicine in which the personnel specialize.[9] Emergency physicians use either length- or weight-based estimation to select the appropriate ETT for intubation.[10] Camera-based laryngoscopy is more effective than direct laryngoscopy in achieving first-pass success in difficult airways.[11]
Media
(Click Image to Enlarge)
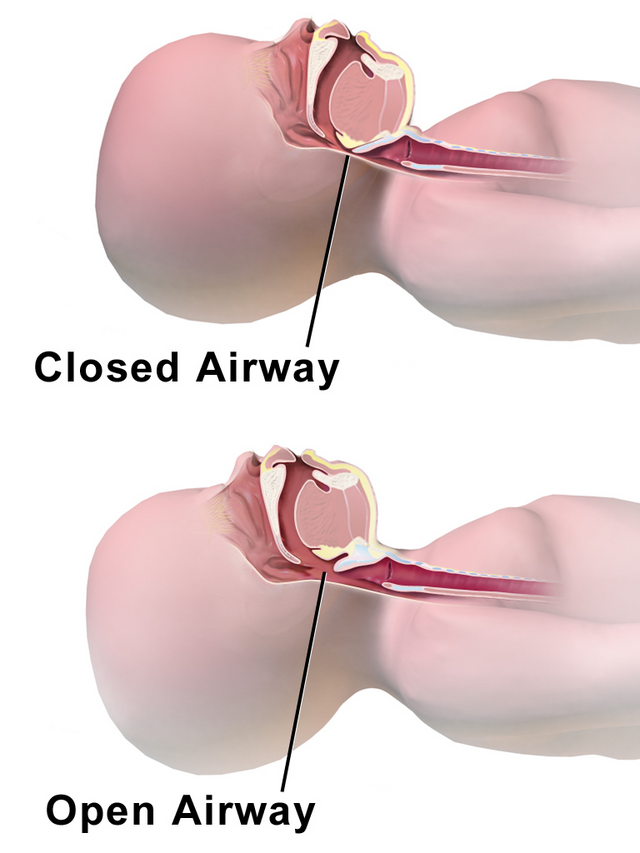
Infant Airway. In the top image, note that the large occiput causes flexion of the head and subsequent obstruction of the upper airway by the tongue base. In the bottom image, this obstruction has been relieved by placing a towel under the shoulders and neck, allowing greater extension of the head and opening of the upper airway.
Blausen.com staff. Medical Gallery of Blausen Medical 2014. WikiJournal of Medicine. doi: 10.15347/wjm/2014.010.
(Click Image to Enlarge)
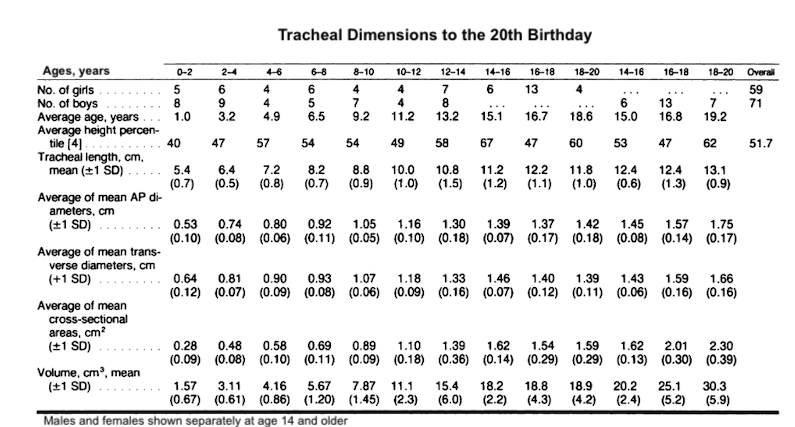
Tracheal Dimensions to the 20th Birthday. Male and female individuals shown separately at age 14 and older.
Adapted from Griscom NT, Wohl MEB. Dimensions of the growing trachea related to age and gender. AJR. 1986;146:233-237.
References
Harless J, Ramaiah R, Bhananker SM. Pediatric airway management. International journal of critical illness and injury science. 2014 Jan:4(1):65-70. doi: 10.4103/2229-5151.128015. Epub [PubMed PMID: 24741500]
Griscom NT, Wohl ME. Dimensions of the growing trachea related to age and gender. AJR. American journal of roentgenology. 1986 Feb:146(2):233-7 [PubMed PMID: 3484568]
Shibasaki M, Nakajima Y, Ishii S, Shimizu F, Shime N, Sessler DI. Prediction of pediatric endotracheal tube size by ultrasonography. Anesthesiology. 2010 Oct:113(4):819-24. doi: 10.1097/ALN.0b013e3181ef6757. Epub [PubMed PMID: 20808208]
Newth CJ, Rachman B, Patel N, Hammer J. The use of cuffed versus uncuffed endotracheal tubes in pediatric intensive care. The Journal of pediatrics. 2004 Mar:144(3):333-7 [PubMed PMID: 15001938]
Piepho T, Kriege M, Byhahn C, Cavus E, Dörges V, Ilper H, Kehl F, Loop T, Raymondos K, Sujatta S, Timmermann A, Zwißler B, Noppens R. German guidelines for airway management 2023. Die Anaesthesiologie. 2024 May 16:():. doi: 10.1007/s00101-024-01413-5. Epub 2024 May 16 [PubMed PMID: 38753159]
Long B, Gottlieb M. Emergency medicine updates: Endotracheal intubation. The American journal of emergency medicine. 2024 Nov:85():108-116. doi: 10.1016/j.ajem.2024.08.042. Epub 2024 Sep 3 [PubMed PMID: 39255682]
Roberts K, Whalley H, Bleetman A. The nasopharyngeal airway: dispelling myths and establishing the facts. Emergency medicine journal : EMJ. 2005 Jun:22(6):394-6 [PubMed PMID: 15911941]
Shen CM, Soong WJ, Jeng MJ, Lee YS, Cheng CY, Sun J, Hwang B. Nasopharyngeal tract length measurement in infants. Acta paediatrica Taiwanica = Taiwan er ke yi xue hui za zhi. 2002 Mar-Apr:43(2):82-5 [PubMed PMID: 12041622]
Davis DP, Koprowicz KM, Newgard CD, Daya M, Bulger EM, Stiell I, Nichol G, Stephens S, Dreyer J, Minei J, Kerby JD. The relationship between out-of-hospital airway management and outcome among trauma patients with Glasgow Coma Scale Scores of 8 or less. Prehospital emergency care. 2011 Apr-Jun:15(2):184-92. doi: 10.3109/10903127.2010.545473. Epub 2011 Feb 10 [PubMed PMID: 21309705]
Daugherty RJ, Nadkarni V, Brenn BR. Endotracheal tube size estimation for children with pathological short stature. Pediatric emergency care. 2006 Nov:22(11):710-7 [PubMed PMID: 17110862]
Level 2 (mid-level) evidenceMosier JM, Stolz U, Chiu S, Sakles JC. Difficult airway management in the emergency department: GlideScope videolaryngoscopy compared to direct laryngoscopy. The Journal of emergency medicine. 2012 Jun:42(6):629-34. doi: 10.1016/j.jemermed.2011.06.007. Epub 2011 Sep 10 [PubMed PMID: 21911279]
Level 2 (mid-level) evidence