Introduction
The word obturator comes from the Latin word obturo, which means “to stop or block up.” This adequately illustrates the location of the obturator muscles since they cover the opening of the obturator foramen. Both the obturator externus and obturator internus are bilateral-triangular shaped muscles. Generally, they originate from the obturator membrane and pelvic bone and attach to the greater trochanter of the femur.[1] They are both considered a part of the muscle group that externally rotates the hip along with gemellus superior and inferior, piriformis, and quadratus femoris.[1] See Image. Pelvic Region Anatomy.
The main functions of the obturator internus are to externally rotate the femur when the hip is extended and abduct the femur when the hip is flexed. Additionally, the obturator internus plays a vital role in stabilizing the femoral head in the acetabulum. As a result, this muscle can be injured or weakened by posterior dislocations of the hip since the bone is driven back into the obturator internus and gluteal muscles. Similar to the obturator internus, the primary function of the obturator externus is to externally rotate the hip. It can assist with this movement when the hip is in either the neutral or flexed position. It has also been shown that this muscle can assist with the adduction of the flexed hip. Due to their function and location, they both can be damaged in sporting activities involving kicking, tackling, and falling. Sprains to these muscles are rare, but when they do occur, young male athletes are most often affected.[2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The obturator externus and internus are bilateral-triangular shaped muscles originating in the pelvis and inserting onto the greater trochanter of the femur. The obturator muscles work synergistically with surrounding muscles to provide hip mobility. Their primary function is external rotation of the hip. In addition, the obturator externus contributes to adduction of the flexed hip, while the obturator internus plays a role in the abduction of the flexed hip. See Image. Hip Anatomy.
The obturator externus originates primarily from the bony margin of the obturator foramen, although it has been shown that some fibers originate from the obturator membrane.[3] The muscle inserts as a cylindrical tendon onto the greater trochanter of the femur. A cadaveric study highlighted that the obturator externus forms a musculotendinous junction at the level of the femoral neck and that the fibers at the inferior margin of the acetabulum act like a sling for the inferior portion of the femoral neck.[3] Additionally, when placing the hip in abduction and external rotation, it was noted that the obturator externus was brought closer to the caudal border of the acetabulum.[3]
Together, these findings suggest that the obturator externus may provide some reinforcement to the hip joint. The location of the obturator externus has also been shown to protect the medial circumflex femoral artery (MCFA). One study's results demonstrated that the obturator externus protected the deep branch of the MCFA from being damaged during hip dislocation in any direction.[4] The obturator internus has 2 points of origin. It originates from both the posterior surface of the obturator membrane and the rami surrounding the obturator foramen and inserts onto the greater trochanter of the femur.[5] In addition to contributing to external rotation and abduction of the hip, a critical function of this muscle is the stabilization of the hip joint. The obturator internus shortens as the hip moves from flexion to extension, which indicates that it provides support to the hip joint during weight-bearing and propulsion activities.[6] It has been well established that the obturator internus is a “postural muscle” that holds the femoral head in the acetabulum.[7] Yoo et al state that due to its role in stabilization, it is frequently monitored in gait analysis and muscle rehabilitation after an injury to the hip joint.
Embryology
The development of the musculoskeletal system begins during the fourth week of development with the formation of a limb bud.[8] Between weeks 4 through 8, bone and muscle further develop [8]. Skeletal muscle, in general, is derived from somites, which are transient structures that come from the embryologic paraxial mesoderm.[8] Each somite contains a myotome from which the muscles derive. Myotomes can be further divided into epaxial or hypaxial portions. Innervation is used to classify a muscle as either epaxial or hypaxial. Epaxial muscles receive innervation from the dorsal roots of the spinal nerves, and hypaxial muscles receive innervation from the ventral roots of the spinal nerves.[9] The obturator muscles both stem from the sacral hypaxial myotome.[10] Unlike cardiac and smooth muscle, skeletal muscle is unique since it is under voluntary control by the organism. Myogenesis of skeletal muscle requires coordination with the lateral plate mesoderm, which gives rise to the neural, vascular, and connective tissue of the extremities.
Blood Supply and Lymphatics
The obturator externus muscle receives blood supply from branches of the obturator and the femoral artery. The anterior branch of the obturator artery travels along the pubic ramus and supplies the obturator externus. The MCFA is the branch off of the femoral artery and also provides vascularization to the muscle. These 2 branches, as well as the posterior branch of the obturator artery, anastomose with one another near the obturator externus muscle.[11] It should be noted that there is some variability in the supply of the anterior branch of the obturator and the MCFA; therefore, the obturator externus can receive vascularization from either one or both of these arteries.[12][13]
The obturator internus muscle receives blood supply from branches of the obturator artery, the gluteal artery, and the pudendal artery. Branches of the obturator artery include the muscular branches which supply the iliacus and iliopsoas muscles, in addition to the obturator internus (see Image. Internal Iliac Branches).[11] The muscular branches of the inferior gluteal artery also provide blood supply to the muscle.[14] Lastly, the gemellar branch and inferior rectal branch of the pudendal artery supply the lateral portion of the obturator internus.[15] Results from a study by Fronhofer et al found significant variation in the branching pattern of the inferior rectal branch to the obturator internus muscle. Their analysis concluded that 31% of cases had one branch to the obturator internus, 43% had 2 branches, 11% had three branches, and 15% lacked a branch from the inferior rectal artery altogether.[15]
Nerves
The posterior branch of the obturator nerve innervates the obturator externus muscle. The obturator nerve is a branch of the lumbar plexus and originates from the L2-L4 spinal nerves (see Image. Lumbar Nerves). Near the obturator foramen, the obturator nerve branches into posterior and anterior divisions.[16] The anterior and posterior divisions provide motor innervation to muscles in the medial compartment of the thigh, which makes the obturator nerve essential for the adduction of the thigh.[17] The anterior division eventually becomes a cutaneous nerve and provides sensory innervation to the upper medial portion of the thigh and parts of the knee and hip.[17]
The obturator internus muscle is innervated by the nerve to the obturator internus. This is a branch of the sacral plexus and originates from the L5-S2 spinal nerves. This nerve also innervates the superior gemellus muscle. However, some variation in the innervation of the superior gemellus muscle has been identified. It was shown that 60.4% of the time, the superior gemellus muscle received dual innervation from the nerve to the obturator internus and the nerve to the quadratus femoris.[18] Additional testing confirmed that the nerve to the obturator internus and the nerve to the quadratus femoris are 2 independent nerves since they take different courses and lack communication.[18]
Muscles
The obturator muscles are considered part of the short external rotators of the hip, along with the gemellus superior and inferior, piriformis, and quadratus femoris. These muscles are innervated by nerves of the sacral plexus (L5-S2), with the exception of the obturator externus, which receives innervation from the lumbar plexus. Similarly to the obturator muscles, the short external rotators of the hip originate from the pelvic region and insert onto the greater trochanter of the femur (see Image. Short External Rotators of the Hip). The muscles in this group sit posteriorly to the pelvic bone. During contraction, the muscles shorten and work synergistically to rotate the femur laterally.
The medial rotators of the hip act as antagonists to the short external rotators. The medial rotators include the gluteus medius and minimus, tensor fasciae latae, and the hip adductors. While the main function of the obturator externus is external rotation, it can provide a small amount of assistance with adduction of the flexed hip. With the exception of the obturator externus, the hip adductors originate from the pubis or ischium and insert into the medial posterior part of the femur bone. The hip adductors include obturator externus, pectineus, gracilis, and adductor brevis, longus, magnus, and minimus. When the hip is flexed, the obturator internus muscle acts as an antagonist to the obturator externus since it plays a role in abduction. The primary hip abductors include the gluteus medius and minimus and the tensor fasciae latae.
Physiologic Variants
The literature has only reported a few physiological variations of the obturator muscles. One study by Pine et al. examined variations in the relationship between the piriformis and obturator internus to better inform piriformis preservation during posterior hip arthroplasty. The tendon crossing angles, location of insertion onto the greater trochanter, and the fusion between tendons prior to insertion were analyzed. It was found that in 10% of cases, the obturator internus and piriformis tendons combined before insertion on the femur.[19] Somewhat related to anatomical variations, it has also been noted that the architectural design of the obturator internus is particularly affected by aging. The literature demonstrates that age-related changes in the structure of the obturator internus led to a decrease in force-generating capability and an increase in muscle fibrosis.[20]
Surgical Considerations
There are 3 main approaches to total hip arthroplasty: the anterior approach, the anterolateral approach, and the posterior approach. During the posterior approach, the short external rotators, such as the obturator internus, often have to be dissected so that the surgeon can access the hip joint. Before dissection occurs, the sciatic nerve should be identified since it is in close proximity to the short external rotators. The piriformis muscle is used most reliably to locate the sciatic nerve since it typically exits near the inferior edge of the piriformis muscle belly.
After identification of the nerve, the short external rotators can be detached and reflected medially. Medial reflection protects the sciatic nerve from injury during the operation; however, if there are variations in the course of the sciatic nerve or variations in the musculotendinous confluence of the piriformis and obturator internus then a false sense of security can be created. Once dissection is complete, the short external rotators are tagged with a suture and repaired at the end of the operation. The literature shows that by performing a soft tissue repair of the short external rotators during closure, postoperative posterior dislocation rates dropped from 4.5% to 0.5%.[21][22][23] However, it was also noted that the soft tissue repair increased the atrophy of the short external rotator muscles.[21][22]
Another surgical consideration related to the obturator externus is the damage to the nerve. Due to its location within the pelvis, the obturator nerve has the potential to become damaged during gynecological surgery, specifically lymphadenectomy for gynecological malignancies.[24] This could potentially weaken the obturator externus since this muscle is innervated by the posterior branch of the obturator nerve. The obturator internus would not be affected by this surgical complication since it is innervated by the nerve to the obturator internus.
Clinical Significance
Due to their close proximity, the obturator muscles are clinically relevant when there is an injury to the hip, such as dislocation. Posterior hip dislocations are the most common type of hip dislocation. They are typically caused when a posteriorly directed force is applied to a flexed knee while the hip is flexed and adducted. This drives the femoral head posteriorly and causes dislocation of the hip. During dislocation, gluteal muscles and short external rotator muscles, such as the obturator internus, can be injured. However, the most common complications from posterior hip dislocation are avascular necrosis and sciatic nerve injury. The deep branch of the MCFA is the primary blood supply of the femoral head. Damage to this vessel dramatically increases the likelihood of avascular necrosis. Studies have shown that the obturator externus plays a vital role in the protection of the deep branch of the MCFA during hip dislocation in any direction.[4] After posterior hip dislocation, hip stabilizer muscles are monitored in gait analysis and muscle rehabilitation.[7] In addition to becoming damaged as a result of hip dislocations, the obturator internus can also become strained from sports that involve kicking, tackling, and falling.[2] These strains are extremely rare, but when they do occur, it is often seen in young male athletes.[2]
One study by Byrne et al examined 2 cases of obturator internus strains and the results found that this strain can happen both acutely or as a result of overuse. Additionally, obturator internus strains can occur in association with adductor longus strains or independently.[2] The obturator externus bursa also has involvement in pathological conditions. A study performed by Robinson et al. analyzed eight cadaver hemipelvises and ten clinical patients with obturator externus bursa enlargement and associated intraarticular hip abnormality to better understand the anatomy of this bursa and its clinical significance.[25] They found that in all ten patients, the enlarged bursa displaced the obturator externus muscle inferiorly. Additionally, they noted that this bursa could act as a posteroinferior communication of the hip joint capsule and could be a site of disease spread.[25]
Lastly, deep gluteal syndrome is a term used to describe the compression of the sciatic or pudendal nerve by a combination of gemelli-obturator syndrome, piriformis syndrome, ischiofemoral impingement syndrome, and proximal hamstring syndrome.[26] Symptoms include pain in the hip, buttock, and posterior thigh due to nerve entrapment.[26] Gemelli-obturator syndrome occurs when the sciatic nerve becomes compressed between the gemellus muscles and obturator internus during passive hip rotation.[27] Treatment for this condition can include rest, non-steroidal anti-inflammatory drugs, gabapentin, muscle relaxants, and physical therapy.[26]
Media
(Click Image to Enlarge)
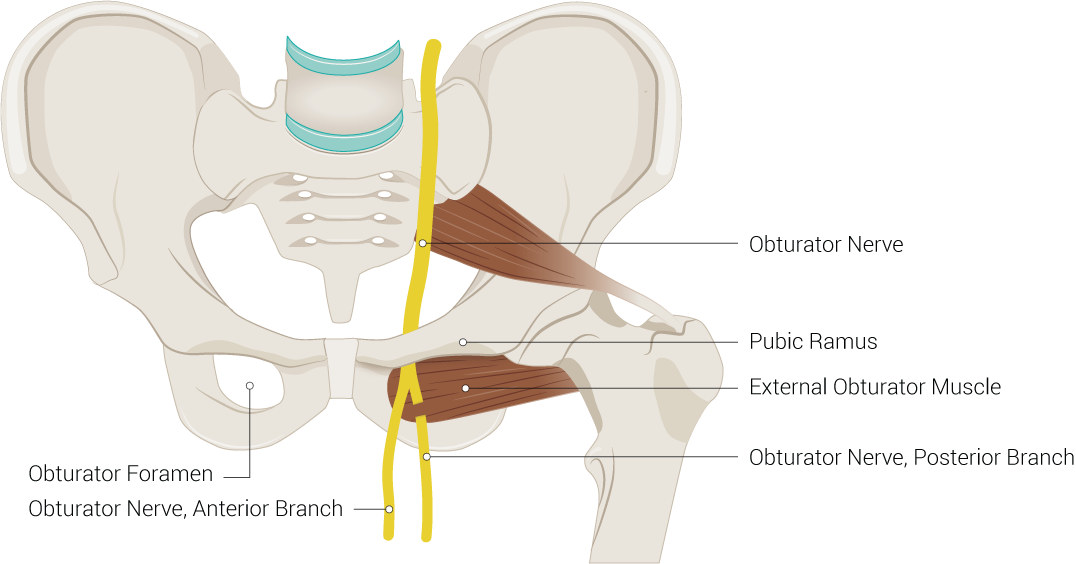
Pelvic Region Anatomy. Illustration includes obturator foramen, pubic ramus, external obturator muscle, obturator nerve, posterior branch, obturator nerve, and anterior branch.
Contributed by B Palmer
(Click Image to Enlarge)
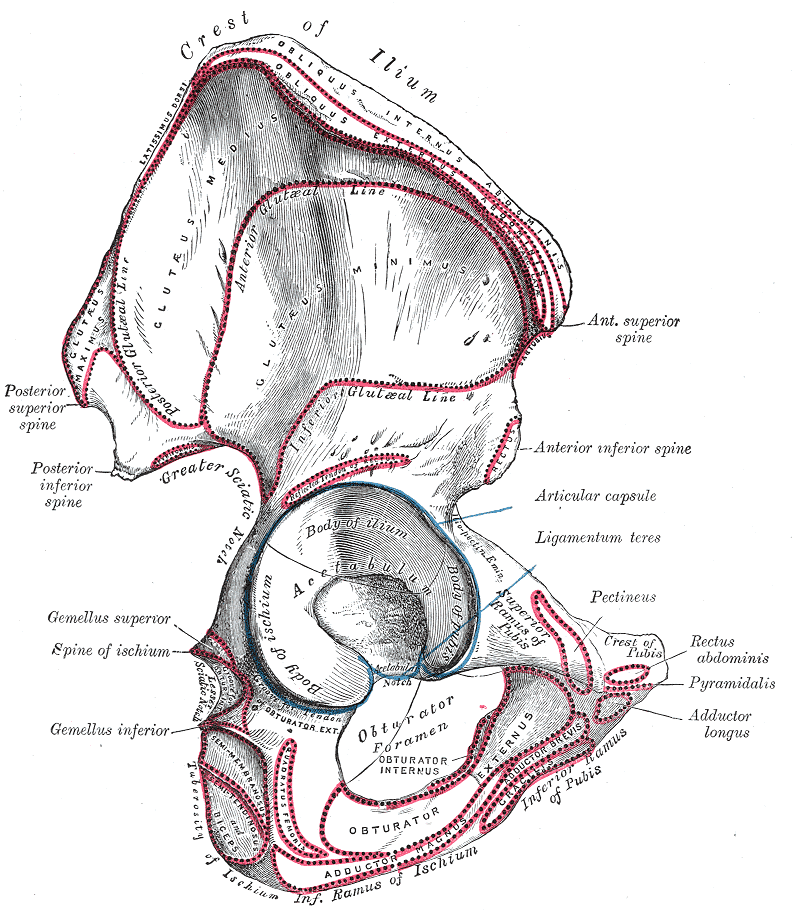
Hip Anatomy. Anatomy includes os innominatum, hip, bone, ilium, crest of ilium, latissimus dorsi, obliquus internus abdominis, obliquus externus abdominis, gluteus maximus, posterior gluteal line, inferior gluteal line, anterior gluteal line, gluteus minimus, posterior superior spine, posterior inferior spine, greater sciatic notch, rectus, anterior superior spine, anterior inferior spine, ligamentum teres, acetabulum, pubis, ischium, gemellus superior, spine of ischium, gemellus inferior, lesser sciatic notch, semimembranosus, semitendinosus, tuberosity of ischium, ramus of ischium, pectineus, crest of pubis, ramus of pubis, adductor brevis, gracilis, obturator foramen, obturator internus, obturator, pectineus, rectus abdominis, pyramidalis, and adductor longus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
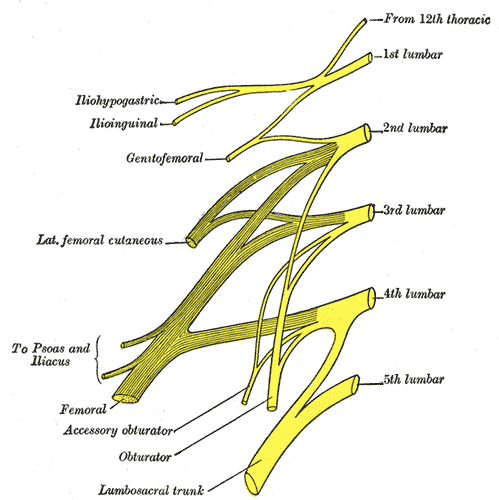
Lumbar Nerves. This illustration depicts the 5 spinal nerves that arise from either side of the spinal cord below the thoracic spinal cord and above the sacral spinal cord.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
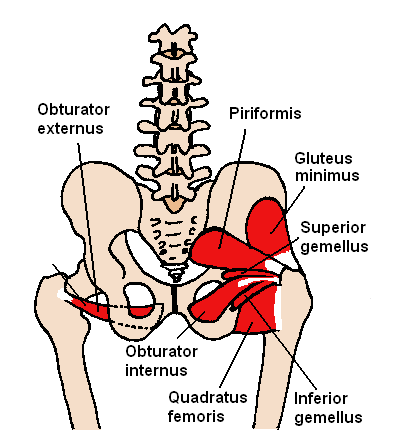
Short External Rotators of the Hip. This illustration shows the short external rotator muscles of the hip, which are composed of 6 postural muscles.
Contributed by B O'hara
(Click Image to Enlarge)
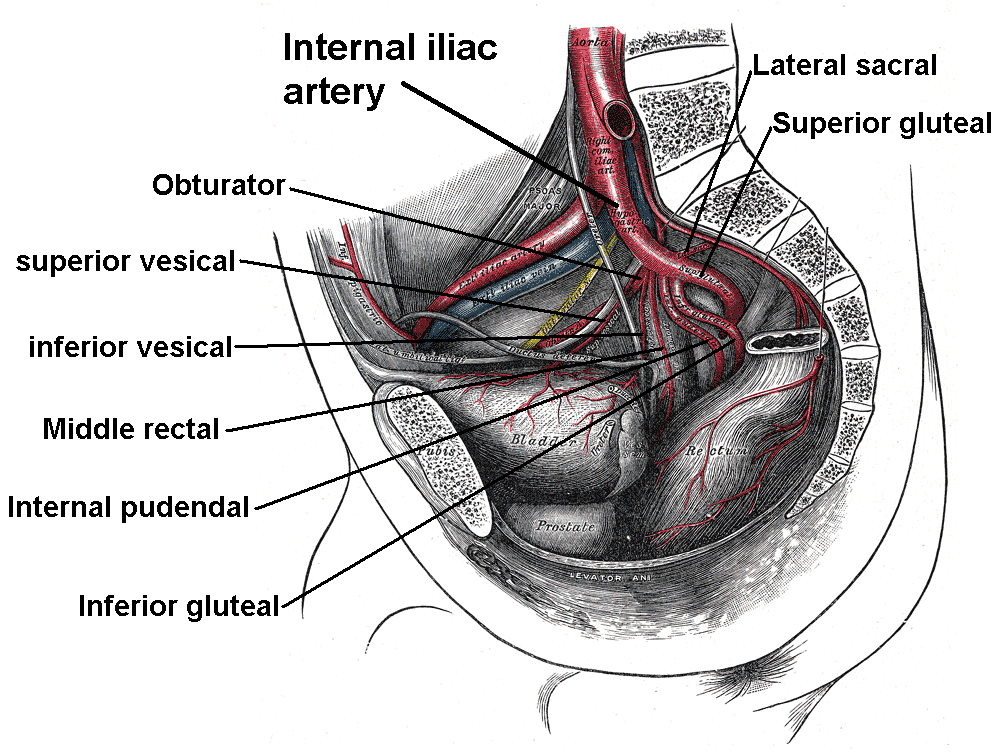
Internal Iliac Branches. This image shows that the internal iliac artery divides into 2 trunks, anterior and posterior. The anterior trunk gives off 8 further branches, while the posterior trunk has 3 branches.
Mikael Häggström, Public Domain, via Wikimedia Commons
References
Kiel J, Kaiser K. Adductor Strain. StatPearls. 2024 Jan:(): [PubMed PMID: 29630218]
Byrne C, Alkhayat A, O'Neill P, Eustace S, Kavanagh E. Obturator internus muscle strains. Radiology case reports. 2017 Mar:12(1):130-132. doi: 10.1016/j.radcr.2016.10.020. Epub 2016 Dec 16 [PubMed PMID: 28228895]
Gudena R, Alzahrani A, Railton P, Powell J, Ganz R. The anatomy and function of the obturator externus. Hip international : the journal of clinical and experimental research on hip pathology and therapy. 2015 Sep-Oct:25(5):424-7. doi: 10.5301/hipint.5000249. Epub 2015 Apr 27 [PubMed PMID: 25952918]
Gautier E, Ganz K, Krügel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. The Journal of bone and joint surgery. British volume. 2000 Jul:82(5):679-83 [PubMed PMID: 10963165]
Khodaee M, Jones D, Spittler J. Obturator Internus and Obturator Externus Strain in a High School Quarterback. Asian journal of sports medicine. 2015 Sep:6(3):e23481. doi: 10.5812/asjsm.23481. Epub 2015 Sep 23 [PubMed PMID: 26448844]
Vaarbakken K, Steen H, Samuelsen G, Dahl HA, Leergaard TB, Nordsletten L, Stuge B. Lengths of the external hip rotators in mobilized cadavers indicate the quadriceps coxa as a primary abductor and extensor of the flexed hip. Clinical biomechanics (Bristol, Avon). 2014 Aug:29(7):794-802. doi: 10.1016/j.clinbiomech.2014.05.011. Epub 2014 Jun 4 [PubMed PMID: 24961540]
Yoo S, Dedova I, Pather N. An appraisal of the short lateral rotators of the hip joint. Clinical anatomy (New York, N.Y.). 2015 Sep:28(6):800-12. doi: 10.1002/ca.22568. Epub 2015 May 30 [PubMed PMID: 26032283]
Chal J, Pourquié O. Making muscle: skeletal myogenesis in vivo and in vitro. Development (Cambridge, England). 2017 Jun 15:144(12):2104-2122. doi: 10.1242/dev.151035. Epub [PubMed PMID: 28634270]
Saberi M, Pu Q, Valasek P, Norizadeh-Abbariki T, Patel K, Huang R. The hypaxial origin of the epaxially located rhomboid muscles. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2017 Nov:214():15-20. doi: 10.1016/j.aanat.2017.05.009. Epub 2017 Jun 26 [PubMed PMID: 28655569]
Naito M, Suzuki R, Abe H, Rodriguez-Vazquez JF, Murakami G, Aizawa S. Fetal Development of the Human Obturator Internus Muscle With Special Reference to the Tendon and Pulley. Anatomical record (Hoboken, N.J. : 2007). 2015 Jul:298(7):1282-93. doi: 10.1002/ar.23121. Epub 2015 Feb 25 [PubMed PMID: 25683268]
Granite G, Meshida K, Wind G. Frequency and Clinical Review of the Aberrant Obturator Artery: A Cadaveric Study. Diagnostics (Basel, Switzerland). 2020 Jul 30:10(8):. doi: 10.3390/diagnostics10080546. Epub 2020 Jul 30 [PubMed PMID: 32751771]
Al-Talalwah W. The medial circumflex femoral artery origin variability and its radiological and surgical intervention significance. SpringerPlus. 2015:4():149. doi: 10.1186/s40064-015-0881-2. Epub 2015 Mar 28 [PubMed PMID: 25883882]
Zlotorowicz M, Czubak-Wrzosek M, Wrzosek P, Czubak J. The origin of the medial femoral circumflex artery, lateral femoral circumflex artery and obturator artery. Surgical and radiologic anatomy : SRA. 2018 May:40(5):515-520. doi: 10.1007/s00276-018-2012-6. Epub 2018 Apr 12 [PubMed PMID: 29651567]
Lung K, Lui F. Anatomy, Abdomen and Pelvis: Superior Gluteal Nerve. StatPearls. 2024 Jan:(): [PubMed PMID: 30571029]
Fronhöfer G, Niernberger T, Anderhuber F. Variations in the branching of the internal pudendal artery in the ischioanal fossa. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 1996 Apr:178(2):133-5 [PubMed PMID: 8638766]
Eickmeyer SM. Anatomy and Physiology of the Pelvic Floor. Physical medicine and rehabilitation clinics of North America. 2017 Aug:28(3):455-460. doi: 10.1016/j.pmr.2017.03.003. Epub 2017 May 27 [PubMed PMID: 28676358]
Koh M, Markovich B. Anatomy, Abdomen and Pelvis, Obturator Nerve. StatPearls. 2024 Jan:(): [PubMed PMID: 31869104]
Aung HH, Sakamoto H, Akita K, Sato T. Anatomical study of the obturator internus, gemelli and quadratus femoris muscles with special reference to their innervation. The Anatomical record. 2001 May 1:263(1):41-52 [PubMed PMID: 11331970]
Level 3 (low-level) evidencePine J, Binns M, Wright P, Soames R. Piriformis and obturator internus morphology: a cadaveric study. Clinical anatomy (New York, N.Y.). 2011 Jan:24(1):70-6. doi: 10.1002/ca.21053. Epub 2010 Nov 10 [PubMed PMID: 21154643]
Cook MS, Bou-Malham L, Esparza MC, Alperin M. Age-related alterations in female obturator internus muscle. International urogynecology journal. 2017 May:28(5):729-734. doi: 10.1007/s00192-016-3167-5. Epub 2016 Oct 4 [PubMed PMID: 27704154]
Setoguchi D, Kinoshita K, Ishimatsu T, Ishii S, Yamamoto T. The short external rotators dissection during the posterior approach in total hip arthroplasty did not change the blood flow. Hip international : the journal of clinical and experimental research on hip pathology and therapy. 2020 Nov:30(6):718-724. doi: 10.1177/1120700019864077. Epub 2019 Jul 11 [PubMed PMID: 31296062]
Kwon MS, Kuskowski M, Mulhall KJ, Macaulay W, Brown TE, Saleh KJ. Does surgical approach affect total hip arthroplasty dislocation rates? Clinical orthopaedics and related research. 2006 Jun:447():34-8 [PubMed PMID: 16741471]
Level 1 (high-level) evidenceIorio R, Specht LM, Healy WL, Tilzey JF, Presutti AH. The effect of EPSTR and minimal incision surgery on dislocation after THA. Clinical orthopaedics and related research. 2006 Jun:447():39-42 [PubMed PMID: 16741472]
Level 2 (mid-level) evidenceTopdagi Yilmaz EP, Topdaği YE, Bilge N, Kumtepe Y. Comparison of the harmonic scalpel with scissors in women who experience obturator nerve injury during lymph node dissection for gynaecological malignancies. Ginekologia polska. 2019:90(10):577-581. doi: 10.5603/GP.2019.0100. Epub [PubMed PMID: 31686414]
Level 2 (mid-level) evidenceRobinson P, White LM, Agur A, Wunder J, Bell RS. Obturator externus bursa: anatomic origin and MR imaging features of pathologic involvement. Radiology. 2003 Jul:228(1):230-4 [PubMed PMID: 12775849]
Park JW, Lee YK, Lee YJ, Shin S, Kang Y, Koo KH. Deep gluteal syndrome as a cause of posterior hip pain and sciatica-like pain. The bone & joint journal. 2020 May:102-B(5):556-567. doi: 10.1302/0301-620X.102B5.BJJ-2019-1212.R1. Epub [PubMed PMID: 32349600]
Balius R, Susín A, Morros C, Pujol M, Pérez-Cuenca D, Sala-Blanch X. Gemelli-obturator complex in the deep gluteal space: an anatomic and dynamic study. Skeletal radiology. 2018 Jun:47(6):763-770. doi: 10.1007/s00256-017-2831-2. Epub 2017 Dec 7 [PubMed PMID: 29218390]