Introduction
Superior oblique myokymia (SOM) is defined as "monocular, high-frequency, low-amplitude, torsional, and involuntary contractions of the superior oblique muscle that result in oscillopsia and diplopia." It is a monocular condition, first described by Duane in 1906 as "unilateral rotary nystagmus." His patient described seeing an object that rose vertically out of the other object and appeared to dance up and down. The term "superior oblique myokymia" was introduced in 1970 by Hoyt and Keane. The condition is now known as superior oblique myokymia of Hoyt and Keane, although the historically more accurate term would be Duane's uniocular micro-tremor. a term that was popular in the 1970s.[1]
History: On the 10th of May, 1906, Alexander Duane saw a 24-year-old woman who complained that over the previous few months, she had episodes of double vision where "the objects appear to dance up and down." On examining the patient, Duane noted intermittent nystagmus, which was limited to the left eye and there were "rapidly repeated, short, quick, to-and-fro oscillations, sometimes mixed (vertical and rotary), at other times purely rotary." He termed it "unilateral rotary nystagmus.
Little progress was made in understanding this condition until 1970, when William Hoyt and James Keane described five patients with similar "hyperactive eye movements" and were the first to suggest that the primary problem was localized to the superior oblique muscle or its nerve. They termed this condition "superior oblique myokymia." Dr. Hoyt noted that the episodes in healthy patients were spontaneous and unilateral with oscillations or fluttering, which resulted in the patients experiencing brief torsional and/or vertical double vision. They noted that the attacks could occur at any time and multiple times a day and could resolve for years and then return. Dr. Hoyt also noted the rapid frequency (12 to 15 Hz) and low amplitude (1 to 2 degrees ) of the vertical and incyclotorsional movements.[2]
He also pointed out the best way to examine for superior oblique myokymia: examining the patient under the slit-lamp and picking out a conjunctival vessel on the eye, which should be watched to detect the intermittent incyclotorsion. This remains the best way to examine these patients. Drs Hoyt and Keane hypothesized that the etiology of SOM included partial denervation of the muscle due to trochlear nerve injury or a pathologic alteration of the membrane threshold of neurons in the trochlear nucleus. They compared it to facial myokymia.
Based on his observations, Dr. Hoyt performed a superior oblique tenotomy and ipsilateral recession of the inferior oblique muscle with a resolution of the symptoms. As many patients experience long periods of remission, he suggested that most patients should be treated just with an assurance that this was a benign condition. He also noted that surgical weakening of the superior oblique was not recommended as the resultant persistent double vision in downgaze after such a procedure was more problematic than the initial intermittent oscillopsia.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
There is no known universal underlying cause of SOM.
Multiple sclerosis: There are two cases of SOM reported in patients who had a family history of multiple sclerosis. Uhtoff phenomenon or sign is the transient worsening of neurological symptoms related to a demyelinating condition like multiple sclerosis when the body is exposed to heat (hot weather, hot bath, exercise, fever). One case has been described where the SOM episodes were triggered by exposure to heat. The patient did not have multiple sclerosis.[3]
Brainstem tumors, lesions of the cerebellopontine angle, and head trauma: cases of SOM have occurred after brainstem tumors and after head or ocular trauma. However, most patients with SOM do not report prior trauma. For example, SOM has been found in a patient with a posterior fossa pilocytic astrocytoma. The symptoms resolved after resection of the tumor. Similarly, SOM has also been seen in a patient with a dural arteriovenous fistula, where the symptoms improved after fistula embolization.[4]
Trauma and superior oblique palsy: SOM has been known to arise in the setting of fourth nerve palsy. Midorbital atrophy of the ipsilateral superior oblique muscle has been shown in a subset of patients with SOM. Trauma snd superior oblique palsy may precipitate SOM but is not universally seen.[5]
Structural compromise of the trochlear nerve by compression or trauma with subsequent aberrant nerve regeneration or ephaptic transmission: Ephaptic transmission is direct transmission across adjacent neural cell membranes that bypass synapses. Other ephaptic transmission conditions include hemifacial spasm, facial synkineses, epilepsy, and ocular neuromyotonia.
Neurovascular compression of the trochlear nerve by an adjacent artery has been shown to cause recurrent attacks of SOM. Bringewald proposed neurovascular compression of the trochlear nerve as a cause of SOM in 1983. Magnetic resonance imaging (MRI) has demonstrated neurovascular compression of the trochlear nerve root at the brainstem exit zone.
More recently, microvascular decompression at the site of compression, first reported by Samii et al. in 1998 and others since, has led to the resolution of SOM. As with hemifacial spasms, MRIs have shown neurovascular compression on the side of the SOM at the root exit of some of the brainstem. Compression is caused by the neighboring superior cerebellar artery. The pontomesencephalic portion of the superior cerebellar artery crosses above the trochlear nerve.
Variations in the anatomy of this vessel are thought to give more likelihood of compression in some patients. It is believed that compression can lead to focal demyelination with resultant susceptibility of the nerve to ephaptic transmission and secondary aberrant signals caused by the disruption of the nerve causing SOM. So SOM may, in some cases, fall under the umbrella of "neurovascular compression syndromes," where the associated cranial nerves result in recurrent symptoms and signs. Examples of such neurovascular compression syndromes include trigeminal neuralgia, hemifacial spasm, ocular neuromyotonia, and vestibular paroxysmia.
Neurovascular compression is thought to result in axonal demyelination, causing the nerve to become susceptible to ephaptic transmission. These neurovascular compression syndromes will demonstrate sudden attacks which can persist in sleep and will show resolution after microvascular decompression.
Although neurovascular compression has been shown to cause SOM, it should be noted that not all cases of SOM have neurovascular compression. It is thought that some cases of SOM may be associated with recovery from trochlear nerve palsy resulting in aberrant nerve regeneration or ephaptic transmission.[6]
Epidemiology
In a comprehensive review of all published cases of superior oblique myokymia, Zhang et al. reviewed the findings in 116 cases and found the following:
- Age at the time of examination ranged from 17 to 72 years (mean 42 years).
- The age of presentation was the same for men and women.
- Half the patients presented between the ages of 31 and 50 years, regardless of sex.
- Most tended to be young, healthy adults.
- SOM more commonly affects the right eye (61%).
- The right-sided predominance was statistically significant in women but not in men.
- The sexes are equally affected.
- SOM was unilateral in all cases.
- In MRI studies, there is no anatomical asymmetry of the trochlear nerve or the superior cerebellar arteries.[7]
Pathophysiology
It is thought that ephaptic transmission of impulses may be responsible for many of the cases seen with superior oblique myokymia.
History and Physical
The patient will complain of double vision or "rotating images" (oscillopsia). The symptoms may be present for a few seconds to hours and generally occur many times a day. Because the symptoms are present with the eyes open, the patient does not complain of any symptoms when asleep. With hemifacial spasms, on the other hand, it will be observed that the spasms are visible even when the patient is asleep.
Triggers: patients will often associate the symptoms with stress, fatigue, nicotine, caffeine, and in one case, heat. In most patients, the symptoms are spontaneous. When the symptoms occur, the patient will be aware of the sensation of an abnormal movement of the eye and will describe double vision and oscillopsia. Although the episodes occur spontaneously, they may be induced by having the patient look in the direction the superior oblique muscle moves the eye: in and down.[8]
Clinical Findings: the movements caused by the superior oblique muscle tend to be of high frequency (up to 50 Hz) and low amplitude (less than 4 degrees). There is torsion of the eye with rapid nystagmic monocular movement (see Videos). There will generally be fast 2 to 3 Hz intorting movements followed by slower extorting of the eye. Although the amplitudes are low (2 - 4 degrees), it is not uncommon to see occasional jerking amplitudes of 5 degrees or more.
Wertenbaker noted an audible phenomenon when two patients were examined with a stethoscope on the affected eye. He described "an irregular, rapid, machine gun sound." Others have not reported this finding, and in three patients, we could not elicit such a sound. Remissions and exacerbations of SOM can last days to weeks, months, and even years.[8]
Extraocular Movements: generally, there are no ocular movement abnormalities on examination, although, in some patients, a slight weakness of the superior oblique muscle may be detected with associated hypertropia, which changes to a hypotropia where there is an episode of spasm. Signs of superior oblique palsy should be looked for: patients will demonstrate ipsilateral hypertropia snd excyclotorsion. Patients may also demonstrate an overshoot of saccades in the downgaze in the affected eye.
Torticollis: subtle torticollis with a contralateral head tilt with a chin down position may occur as the patient tries to position the head where the oscillations are least troublesome.[9]
Evaluation
Electromyography: most patients are not subjected to electromyographic tests. However, electromyography demonstrates high-voltage discharges which are prolonged.[10][11]
Contrast-enhanced magnetic resonance imaging (MRI): all patients presenting with SOM are not investigated with MRI as the yield of brainstem tumors is low. However, patients who do not respond to medical treatment and present with intractable symptoms or worsening symptoms should undergo neuroimaging with specific MRI protocols (flow imaging using steady acquisition -FIESTA, or constructive interference in steady-state sequence - CISS) with imaging through the midbrain.[12]
Magnetic resonance angiography is also requested, looking for vascular compression of the root of the trochlear nerve. This neuroimaging will detect posterior cerebellar artery compression of the trochlear nerve and detect tumors or signs of prior trauma.[12]
Treatment / Management
No definitive treatment has been recognized for SOM. Most patients with SOM will present to the ophthalmologist because of the visual symptoms. The variable symptoms and periods of remission make definitive treatment assessment difficult. Furthermore, it is a rare condition, with less than 200 cases reported.
Medications: successful treatments have included topical beta-blockers, carbamazepine, baclofen, clonazepam, memantine, mirtazapine, and phenytoin. All these medications are thought to work because of their membrane-stabilizing effects)[13]
- Carbamazepine administered in a dose of 200 mg two to four times a day has been shown to give a substantial improvement or complete resolution of symptoms in SOM in 80% of patients. Side-effects of carbamazepine may limit the use of the drug. Side effects include rash, anemia, hyponatremia, and elevated liver enzymes.[14]
- White et al. found that 80% of 20 patients with SOM successfully responded to systemic medical treatment, including carbamazepine, propranolol, phenytoin, and baclofen.
- Topical beta-blockers such as timolol, levobunolol, and betaxolol, as well as systemic propranolol, have been shown to be successful. Oral propranolol at a dose of 10 mg daily was found to be useful for a patient with SOM. It is thought that beta-blockers reduce the blood pressure amplitude, thereby reducing the pulsatile compression of the trochlear nerve. Beta-blockers may also reduce ephaptic transmission by reducing neuronal sensitivity. Zand et al. found that intermittent use of topical levobunolol 0.5% controlled SOM symptoms in two cases with as little as one drop of levobunolol every three weeks: this reduced the intensity of the myokymia but did not eliminate the movements. They succeeded in treating one patient who had had symptoms for 60 years and could discontinue the topical beta-blockers without recurrence. Their other patient had the symptoms controlled with only one to two drops a day every one to two months. This patient had had symptoms several times a day for 13 years. (B3)
As the topical and systemic medications have minimal side effects and as most of these patients initially present to ophthalmologists, these medications are usually the first line of treatment.
Botulinum toxin injection: under myographic control, it is possible to inject the superior oblique muscle with botulinum toxin. However, it is difficult to do this without affecting the adjacent muscles and causing a superior oblique weakness with resultant double vision. While involved in the care of 3 patients with Mr. John Lee at Moorfields Eye Hospital in London with SOM, we observed limited success with botulinum toxin injections with persistent vertical diplopia for several months in each patient and involvement of the medial rectus in two. As a result, the use of botulinum toxin for SOM has largely been abandoned.[15]
Surgery: Surgery may be considered when patients fail to respond to medical treatments or get a recurrence of intractable symptoms.[16]
Superior oblique muscle surgery: Hoyt performed a superior oblique tenotomy and ipsilateral recession of the inferior oblique muscle with a resolution of the symptoms described in his first report. Subsequently, procedures have included superior oblique tenotomy, superior oblique myectomy, superior oblique myectomy with trochlectomy, and ipsilateral inferior oblique muscle weakening to overcome the inevitable superior oblique weakness created by these procedures. Some patients have required a contralateral inferior rectus muscle procedure because of the diplopia created by the superior oblique muscle weakening procedure.
Currently, the procedure of choice combines a superior oblique tenotomy with ipsilateral inferior oblique myectomy, as first performed and described for this condition by Hoyt in 1970. Agarwal and Kushner found that more than a third of these patients undergoing surgery had residual vertical double vision requiring prisms or further surgery. Superior oblique myokymia may persist even after superior oblique tenotomy because of tendon remnants or fascial or sheath connections, which may heal after surgery.
Parks has observed that complete elimination of the function of the superior oblique muscle may not occur even after tenectomy. Because of this, Ruttum and Harris recommended the removal of the trochlea as well as a 10 mm segment of the superior oblique muscle via an anterior orbitotomy approach. Diplopia occurs in downgaze in nearly half the patients undergoing superior oblique tenectomy, although most patients do not develop hypertropia in the primary gaze, which is surprising. This may be because most of these patients underwent inferior oblique myectomy at the same time as the superior oblique tenectomy.
Law et al. successfully performed an ipsilateral superior rectus recession in a case with persistent myokymia after tenectomy and needed resection of residual fibers. The patient had hypertropia following an initial surgery that resolved with the superior rectus recession, which is an unconventional approach to hypertropia, normally treated with a contralateral inferior rectus recession.
Partial superior oblique tendon weakening: this has been termed the reverse 'Harada-Ito" procedure, where the anterior fibers of the superior oblique tendon are weakened, preserving the remaining superior oblique tendon fibers, thereby preserving some of the superior oblique function. Komorsky et al. treated one patient in this manner by nasally transposing the anterior fibers of the superior oblique tendon. Partial anterior tenectomy may also eliminate symptoms, but this procedure has not been reported to date.
With any procedure that preserved part of the superior oblique tendon insertion, some symptoms may persist, albeit being less troublesome. Conversely, any tenectomy or complete tenotomy procedure is likely to lead to some degree of double vision and would require further surgery to the ipsilateral inferior oblique muscle and sometimes the contralateral inferior rectus muscle. When proposing superior oblique muscle and tendon surgery, these details need to be discussed with the patient.
Microvascular decompression: Samii et al. described the first case of surgical decompression of the trochlear nerve in 1998. A Goretex or Teflon graft is inserted between the offending artery and the trochlear nerve. The arterial loop usually arises from the superior cerebellar artery and affects the nerve at the root entry zone, causing axonal compression. Intraoperative electromyography showed the erratic axonal discharge causing SOM, which stopped following the placement of a Teflon graft.
There have subsequently been a total of six cases described in the literature using different neurosurgical approaches. Half the patients had postoperative trochlear nerve palsy that lasted from weeks to months but recovered. The procedures were curative of the symptoms of SOM. The commonest surgical approach has been the retrosigmoidal approach. Kawasaki et al. have suggested that the lateral superior cerebellar approach gives a better operative view allowing fine manipulation of the vessel and the nerve for decompression. In the retrosigmoidal approach, there is no retraction of the cerebellum, and this may limit the operative view.
Neurosurgical microvascular decompression of the trochlear nerve root is reserved for patients with intractable symptoms not alleviated with medial treatments or focal superior oblique tendon and muscle surgery. Such patients should always undergo neuroimaging to look for vascular anomalies in the vicinity of the origin of the trochlear nerve and also to exclude brainstem tumors.[12](B2)
History of the neurovascular compression theory: The neurovascular compression theory was proposed by Peter Jannetta when he was a neurosurgery resident at the University of California. In 1965, while performing cranial nerve microdissections for dental students, Jannetta identified the trigeminal portio intermedia. He proposed that preserving these sensory fibers may avoid the facial numbness that was common after surgery for trigeminal neuralgia. He and Robert Rand developed a subtemporal transtentorial approach to achieve selective rhizotomy for trigeminal neuralgia.
As such surgery would be forbidden for a resident to perform at the University of California hospital, he operated on a patient with John Alksne at the Harbor General Hospital. On seeing the trigeminal nerve compression by the superior cerebellar artery at surgery, he said, "that's the cause of the tic." He proposed that alleviating the compression of the nerve may be curative.
Some months later, when examining a patient with hemifacial spasm, it occurred to Jannetta that a similar microvascular compression could cause this condition. He went on to perform the first Jannetta microvascular decompression procedure on this patient with success. The neurosurgical cognoscenti of the time were not inclined to accept such radical theories from a resident.
Over decades, the refinement of his surgical technique and presenting his results led to the acceptance of microvascular decompression surgery for trigeminal neuralgia and hemifacial spasm. It is considered one of the great advances in neurosurgeries, and the approach is now applied to other conditions such as SOM and glossopharyngeal neuralgia. Interestingly, the concept of compression of nerve roots by normal vessels was introduced by Dandy and Gardner. Indeed, Dandy had been able to identify compression of the trigeminal nerve root by the superior cerebellar artery loop in 30.7% and compression by a branch of the petrosal vein in 14% of the 215 cases he presented in 1934. This was prior to the use of microscopes.
Interestingly, he did not consider separating the compressing vessels from the nerve. Gardner, in 1962 reported placing a gel foam pad between a compressing artery and nerve in cases of trigeminal neuralgia and hemifacial spasm.
Management algorithm: Based on a review of the cases described in the literature and the results of medical and surgical interventions, the logical management of SOM would be as follows:
- A patient diagnosed with SOM but is asymptomatic or minimally symptomatic: no treatment prescribed and watchful waiting.
- A patient diagnosed with SOM and who is symptomatic: trial of topical beta-blockers like timolol, betaxolol, levobunolol. A gradual reduction in the dose, even down to treatment every few weeks, is tried if the patient responds to treatment.
- A patient diagnosed with SOM is symptomatic and has not responded to topical beta-blockers: trial of medical treatments such as baclofen, gabapentin, carbamazepine, or memantine. These patients can be weaned off these drugs over time.
- A patient diagnosed with SOM is symptomatic and has not responded to topical beta-blockers or systemic medications: obtain neuroimaging prior to offering any surgery. The least invasive surgery with the fewest side effects should be undertaken. Consider partial weakening of the superior oblique tendon. The patient may need ipsilateral inferior oblique myectomy, depending upon the degree of superior oblique muscle weakening.
- A patient diagnosed with SOM is symptomatic and has intractable symptoms with failure of the above treatments; obtain proper neuroimaging looking for vascular compromise of the trochlear nerve. Consider neurosurgical neurovascular decompression.[16]
Differential Diagnosis
Inferior oblique myokymia: Inferior oblique myokymia is a rare condition described by Chinskey and Cornblath in 2013. The eye demonstrates excyclotorsion as opposed to incyclotorsion seen in SOM. The excyclotorsion can be induced by the supraduction of the eye.
Alternating superior and inferior oblique myokymia: Smith and Cornblath described a case of alternating superior and inferior oblique myokymia in 2014 where there were monocular, high-frequency, low-amplitude contractions with incyclotorsion and excyclotorsion of the eye, suggesting alternating superior and inferior oblique myokymia.[17]
Eyelid myokymia: Although the clinical features of SOM are very distinctive, eyelid myokymia, where patients note contractions of the orbicularis oculi muscle, may result in the patient noting a vision change. This is caused by the pressure of the eyelid against the globe as the muscle fibers contract and is not true oscillopsia or double vision. Clinical examination will reveal the fine high-frequency fasciculations of the orbicularis oculi muscle affecting the upper or the lower eyelid. Eyelid myokymia is said to be triggered by fatigue, stress, or caffeine intake, but the exact cause of the condition is unknown. Eyelid myokymia may occur for several hours to days and persist for many weeks. Most will resolve spontaneously, but some require local botulinum toxin injection.
The Heimann-Bielschowsky phenomenon: This phenomenon is seen in patients with reduced vision in an eye. There is monocular vertical eye movement with low-frequency and pendular vertical oscillations of the eye. There are no associated neurological conditions with this phenomenon. In SOM, the oscillations have a low amplitude (less than 4 degrees) and high frequency (up to 50 Hz), whereas in the Heimann-Bielschowsky phenomenon, the frequency is low (less than 5Hz) and the amplitude is high (possibly up to 30 degrees).[18]
Square wave jerks: These are low-amplitude eye movements with high frequency and occur with central neurological lesions that cause fixation instability. Patients may be asymptomatic but may also describe side-to-side image movements. In contrast, SOM patients describe images that bounce up and down. The movements in square wave jerks are usually horizontal and saccadic in nature.
Ocular neuromyotonia: Sudden and episodic contraction of one or more extraocular muscles may occur. This is often associated with radiation injury and is also thought to be caused by ephaptic transmission with injury to the nerve lining. Ocular neuromyotonia may be monocular or binocular, and any extraocular muscles may be involved, including the superior oblique muscle. However, the spasms are slower than those seen with SOM, and involvement of just the superior oblique muscle alone is rare. Ocular neuromyotonia is usually triggered by an eccentric gaze.
Pertinent Studies and Ongoing Trials
Jannetta was of the opinion that even patients who did not show clear neuroimaging findings of compression of the facial nerve might respond to neurosurgical, neurovascular decompression in patients with hemifacial spasms. There have only been a handful of patients with SOM who have undergone neurosurgical decompression, although all achieved success.
As more clinical information is collected, it will be interesting to see if the same mandate will apply to SOM and where most patients with intractable symptoms will respond to neurosurgical, neurovascular decompression of the trochlear nerve.
Prognosis
Most patients with SOM will present with symptoms of "trembling vision" or double vision. As the symptoms vary significantly, many patients may not require any treatment. The majority of patients treated with topical beta-blockers with or without systemic medications will respond with a reduction or elimination of symptoms. Some patients will need superior oblique tendon surgery, with or without ipsilateral inferior oblique surgery, to reduce or eliminate the symptoms. Finally, the few patients with intractable symptoms should be considered for neurosurgical decompression surgery. Although invasive and with risks, the procedure has to date, shown to be very effective.
Complications
Many patients undergoing superior oblique tendon weakening procedures will develop double vision (more than a third of the patients). These patients will need further extraocular muscle surgery to control the double vision or will need to wear prisms. Too few patients have undergone neurosurgical, neurovascular decompression to allow assessment of complications of this procedure, although half of the patients developed fourth nerve palsy following surgery which resolved over weeks to months. All neurosurgical procedures carry morbidity and mortality.
Deterrence and Patient Education
It is important to educate the patient about the condition of superior oblique myokymia: in most cases, there is no underlying cause that needs to be treated. Brainstem tumors and cerebellopontine tumors are very rarely the cause of SOM. Most patients with minimal symptoms should be given no medical or surgical treatment. Those with troublesome symptoms should be guided by the treatment algorithm discussed above.
Pearls and Other Issues
- Superior oblique myokymia presents with episodic unilateral low-amplitude and high-frequency torsional and vertical movements of the eye with associated binocular vertical double vision and unilateral oscillopsia.
- The clinical findings may be subtle, so it is not uncommon for patients to have been seen by several physicians before a correct diagnosis of SOM is made.
- SOM should be suspected when examining any patient with a history of intermittent unilateral oscillopsia or binocular double vision.
- Interval examinations may be necessary because of the episodic nature of SOM.
- The diagnosis may be missed if the patient is not examined carefully on the slit lamp.
- It is thought that SOM occurs because of altered membrane thresholds of the trochlear nerve, resulting in the ephaptic transmission of impulses. Compression of the trochlear nerve by an artery is seen in some patients.
- Patients who do not respond to medical treatment should be investigated with contrast-enhanced MRI studies.
- A substantial number of patients with SOM will require no treatment.
- Response to topical beta-blockers and other systemic medications is excellent in most patients.
- Surgical intervention with surgery to the superior oblique tendon should be undertaken by experienced strabismologists who have experience operating on the superior and inferior oblique muscles.
- Specialized teams should only take neurosurgical intervention with experience in the rare neurovascular surgical decompression procedure.
Enhancing Healthcare Team Outcomes
Optometrists and ophthalmologists should be educated about the condition of superior oblique myokymia, which is rare but can cause significant symptoms in some patients. An accurate diagnosis requires understanding how to examine the patient as the diagnosis is clinical. Based on the history and severity of findings, ophthalmologists, strabismologists, neurologists, neuro-ophthalmologists, and neurosurgeons may need to be involved with the patient's care. The ophthalmologist should be the primary physician providing care and guiding the patient through the treatments. [Level 3]
Media
(Click Video to Play)
(Click Video to Play)
(Click Image to Enlarge)
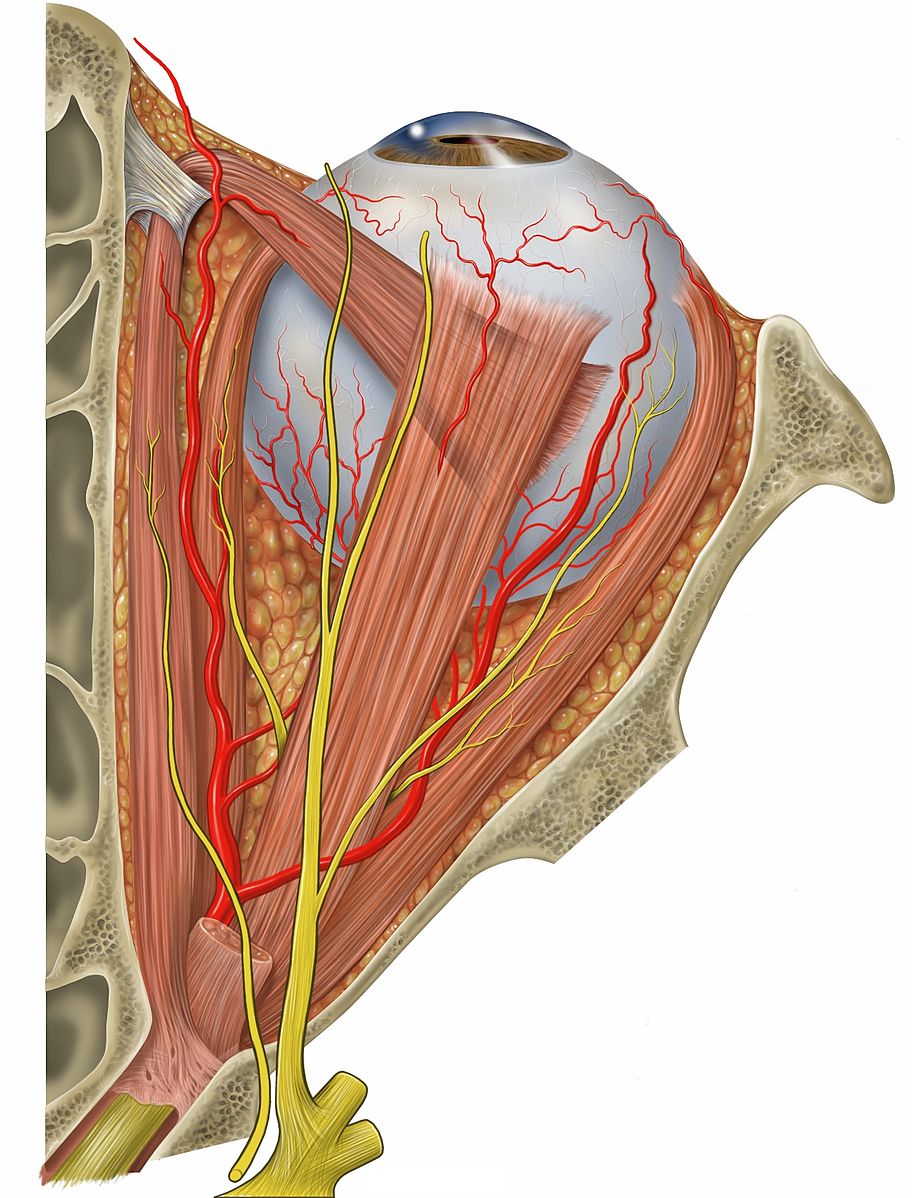
Superior Oblique Myomymia: Anatomy of the Superior Oblique Muscle. The muscle changes direction via the trochlea which is a pulley-like structure and passes under the superior rectus muscle and inserts posteriorly and temporally on the globe. Muscle action causes intorsion and depression of the eye. Contributed by Prof. Bhupendra C. K. Patel MD, FRCS with the creative commons license (Creative Commons Attribution 2.5 License 2006) https://en.wikipedia.org/wiki/File:Eye_orbit_anatomy_superior.jpg Patrick J. Lynch, medical illustrator
(Click Image to Enlarge)
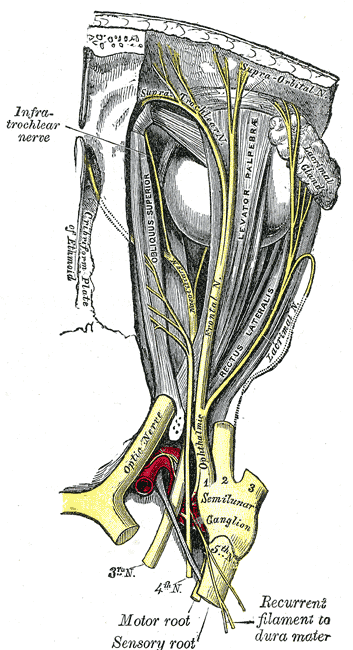
Superior Oblique Myomymia: Innervation of the extra ocular muscles, the lacrimal gland and the sensory nerves of the orbit. Note that the muscular superior oblique that runs forwards in the medial orbit becomes a tendon as it passes through the trochlea and then is purely tendinous as it inserts into the posterolateral part of the globe. It is this anterior tendon that is manipulated and operated upon with partial or total tenectomy. Contributed by Prof. Bhupendra C. K. Patel MD, FRCS with the creative commons license (Creative Commons Attribution) https://commons.wikimedia.org/wiki/File:Gray776.pngSuperior Oblique Myomymia: Anatomy of the Superior Oblique Muscle. The muscle changes direction via the trochlea which is a pulley-like structure and passes under the superior rectus muscle and inserts posteriorly and temporally on the globe. Muscle action causes intorsion and depression of the eye. Patrick J. Lynch, medical illustrator
(Click Image to Enlarge)
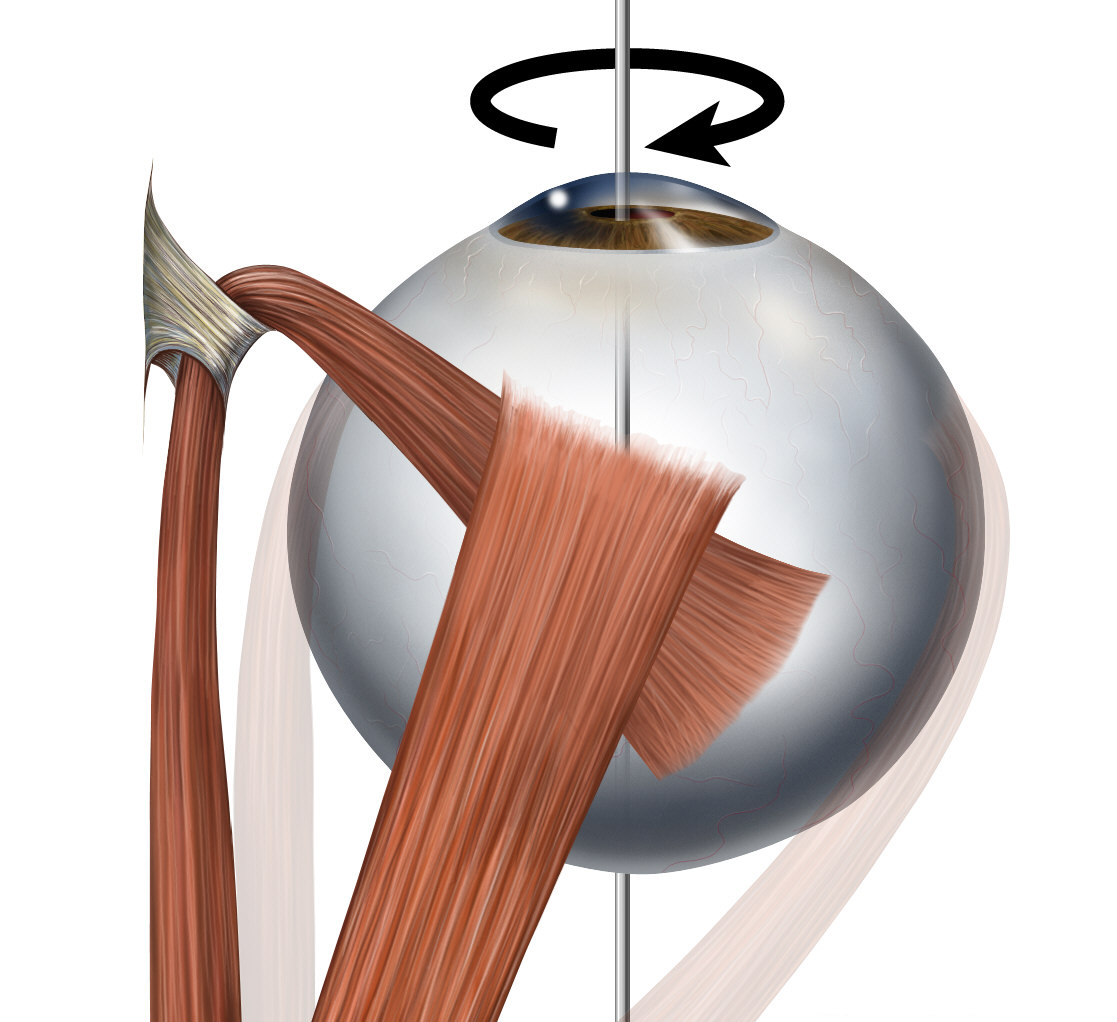
Superior Oblique Myomymia: Action of the Superior Oblique Muscle. The muscle changes direction via the trochlea which is a pulley-like structure and passes under the superior rectus muscle and inserts posteriorly and temporally on the globe. Muscle action causes intorsion and depression of the eye. Contributed by Prof. Bhupendra C. K. Patel MD, FRCS with the creative commons license (Creative Commons Attribution 2.5 License 2006) https://en.wikipedia.org/wiki/Superior_oblique_muscle#/media/File:Eye_movements_lateral_rot.jpg Patrick J. Lynch, medical illustrator
References
Thoorens V, Signolles C, Defoort-Dhellemmes S. [Superior oblique myokymia: a report of three cases]. Journal francais d'ophtalmologie. 2012 Apr:35(4):284.e1-4. doi: 10.1016/j.jfo.2011.05.011. Epub 2011 Dec 2 [PubMed PMID: 22137680]
Level 3 (low-level) evidenceRasool N, Hoyt CS. William F. Hoyt and the Neuro-Ophthalmology of Superior Oblique Myokymia and Ocular Neuromyotonia. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2020 Sep:40 Suppl 1():S29-S34. doi: 10.1097/WNO.0000000000001004. Epub [PubMed PMID: 32796343]
Vighetto A, Tilikete C. [Motorocular syndromes due to neurogenic hyperactivity and their treatment]. Neuro-Chirurgie. 2009 Apr:55(2):272-8. doi: 10.1016/j.neuchi.2009.01.013. Epub 2009 Mar 12 [PubMed PMID: 19285325]
Kishimoto S,Morita S,Kurimoto C,Kitahara C,Tsuji T,Uraki S,Takeshima K,Furukawa Y,Iwakura H,Furuta H,Nishi M,Matsuoka TA, Hypopituitarism and cranial nerve involvement mimicking Tolosa-Hunt syndrome as the initially presenting feature of diffuse large B-cell lymphoma: a case report. BMC endocrine disorders. 2022 Mar 14 [PubMed PMID: 35287660]
Level 3 (low-level) evidenceOh SY. Clinical outcomes and etiology of acquired sixth cranial nerve palsy. Medicine. 2022 Mar 18:101(11):. pii: e29102. doi: 10.1097/MD.0000000000029102. Epub [PubMed PMID: 35356946]
Level 2 (mid-level) evidenceZhang M, Gilbert A, Hunter DG. Superior oblique myokymia. Survey of ophthalmology. 2018 Jul-Aug:63(4):507-517. doi: 10.1016/j.survophthal.2017.10.005. Epub 2017 Oct 19 [PubMed PMID: 29056504]
Level 3 (low-level) evidenceHörner R, Kassubek J, Dreyhaupt J, Ludolph AC. The spectrum and differential diagnosis of acquired ocular motor nerve palsies: a clinical study of 502 patients. Journal of neurology. 2022 Apr:269(4):2140-2148. doi: 10.1007/s00415-021-10761-w. Epub 2021 Sep 19 [PubMed PMID: 34537871]
Cha EH, Ha SG, Suh Shu Y, Kim SH. Clinical features of excyclotorsion in the non-paretic eye of patients with congenital unilateral superior oblique palsy. BMC ophthalmology. 2022 Mar 16:22(1):126. doi: 10.1186/s12886-022-02339-5. Epub 2022 Mar 16 [PubMed PMID: 35296286]
Chung SA, Yim SY, Park A. Sternocleidomastoid muscle asymmetry in unilateral congenital superior oblique palsy. Eye (London, England). 2021 Jul:35(7):1954-1960. doi: 10.1038/s41433-020-01205-2. Epub 2020 Sep 30 [PubMed PMID: 32999476]
Hoyt WF, Keane JR. Superior oblique myokymia. Report and discussion on five cases of benign intermittent uniocular microtremor. Archives of ophthalmology (Chicago, Ill. : 1960). 1970 Oct:84(4):461-7 [PubMed PMID: 5492451]
Level 3 (low-level) evidenceKommerell G, Schaubele G. Superior oblique myokymia. An electromyographical analysis. Transactions of the ophthalmological societies of the United Kingdom. 1980:100(4):504-6 [PubMed PMID: 6947598]
Level 3 (low-level) evidenceNoro S, Seo Y, Honjo K, Okuma M, Asayama B, Amano Y, Kyono M, Hashimoto M, Hanai K, Nakamura H. Lateral Supracerebellar Infratentorial Approach for Superior Oblique Myokymia: A Case Series. Operative neurosurgery (Hagerstown, Md.). 2022 Mar 1:22(3):101-105. doi: 10.1227/ONS.0000000000000015. Epub 2021 Dec 31 [PubMed PMID: 35234412]
Level 2 (mid-level) evidenceMettu P, Mancini R, Friedman DI, Garrity JA. Trochleaectomy: An Effective Treatment of Trochlear Pain in Monocular Patients. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2021 Jun 1:41(2):246-250. doi: 10.1097/WNO.0000000000000916. Epub [PubMed PMID: 32108117]
Joosten IBT, Hoeijmakers JGJ. Mystery Case: Superior oblique myokymia: An uncommon cause of intermittent diplopia. Neurology. 2018 Feb 27:90(9):e814. doi: 10.1212/WNL.0000000000005028. Epub [PubMed PMID: 29483324]
Level 3 (low-level) evidenceDagi LR, Elhusseiny AM. Adjustable graded augmentation of superior rectus transposition for treatment of abducens nerve palsy and Duane syndrome. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2020 Oct:24(5):268.e1-268.e7. doi: 10.1016/j.jaapos.2020.05.013. Epub 2020 Sep 22 [PubMed PMID: 32977023]
Godts DJM, Deboutte IVA, Prinsen S, De Veuster I, Mathysen DGP. Inferior Oblique Recession with 5 mm Loop to Correct Vertical Deviation and Inferior Oblique Overaction Secondary to Superior Oblique Palsy. Journal of binocular vision and ocular motility. 2021 Jul-Sep:71(3):83-89. doi: 10.1080/2576117X.2021.1929788. Epub 2021 Jun 7 [PubMed PMID: 34097575]
Smith TA, Cornblath WT. Alternating superior and inferior oblique myokymia. JAMA ophthalmology. 2014 Jul:132(7):898-9. doi: 10.1001/jamaophthalmol.2014.366. Epub [PubMed PMID: 25010174]
Level 3 (low-level) evidenceAnagnostou E, Karathanasis D, Evangelopoulos ME. The Heimann-Bielschowsky phenomenon after optic neuritis. Multiple sclerosis and related disorders. 2022 Feb:58():103523. doi: 10.1016/j.msard.2022.103523. Epub 2022 Jan 11 [PubMed PMID: 35042093]