Introduction
Siderosis bulbi refers to the pigmentary, degenerative process of the eye following chronic retention of an iron-containing intra-ocular foreign body (IOFB). It can also occur due to iron derived from the blood.[1] First described by Bunge in 1890, siderosis bulbi has an affinity for ocular structures of epithelial origin, such as the cornea, iris, lens, trabecular meshwork, and retina. Iron deposition at these sites leads to the altered morphology of the tissues.[2] A comprehensive clinical evaluation is thus vital to detect the development of ocular siderosis promptly and effectively manage these patients without delay.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Siderosis bulbi occurs due to intra-ocular retention of an iron-containing foreign body. A hammer and chisel injury is the most common mechanism in 41.7% to 59% of cases. Other less frequent mechanisms include gunshot injuries, electric welding, injury due to nail guns, explosion injuries, and road traffic accidents.[3][4][5][6]
Epidemiology
Metallic foreign bodies account for 78% to 86% of cases of all IOFBs, with iron being the most common, followed by lead.[4][7][8] The majority of these patients are middle-aged males. The most common site of entry of an IOFB is the cornea (82.9%), followed by the sclera (11.4%) and the limbus (5.7%).[8] The most common location of an intraocular foreign body lodged in the posterior segment is intravitreal (61%), followed by intra-retinal (14%) and sub-retinal(5%).[9][10][11][6] See Image. Intraocular Foreign Body Following a Penetrating Injury.
Pathophysiology
Oxidative stress, excitotoxicity, and calcium influx play an important role in the pathogenesis of iron-induced retinal toxicity.[12] Two mechanisms of siderosis bulbi have been postulated in the literature, namely, direct and indirect siderosis bulbi. Direct siderosis primarily occurs due to the hydroxyl radical formation following Fenton’s reaction (Fe + HO → Fe + HO• + OH).[13] This results in excessive glutamate accumulation due to inhibition of the reuptake of glutamate by oxygen free radicals. Glutamate leads to the activation and opening of the ligand-gated calcium ion channels and triggers calcium ion influx within the cells with the resultant activation of calcium-dependent enzymes. Ultimately, this leads to irreversible retinal damage involving the degeneration of photoreceptors and retinal pigment epithelium (RPE). Bruch’s membrane and the choroid are spared in the early phase.[14]
Indirect siderosis is due to tissue destruction occurring at sites distal to the IOFB. It involves the retinal vasculature causing toxic microvasculopathy, termed vascular siderosis. This happens due to the affinity of iron for acid mucopolysaccharides that can result in subsequent degeneration of inner retinal layers supplied by capillaries of the central retinal artery. Additionally, damage to RPE cells can occur indirectly by migrating iron ions via vitreous to aqueous through the trabecular meshwork into the suprachoroidal space. Ultimately, from here, the ions diffuse across the choroid and Bruch’s membrane to reach RPE.[15][13] Eventually, all retinal layers get involved in chronic ocular siderosis with the involvement of photoreceptors and RPE in the early direct phase and the inner retinal layers in the indirect form of siderosis.[16]
History and Physical
A detailed history and meticulous evaluation play a vital role in ruling out IOFB in ocular trauma. The initial presenting features of siderosis bulbi include a gradual progressive diminution of vision and night blindness.[1] The patient may also present with dyschromatopsia or progressive scotomas.[13] A Seidel’s test must be performed to detect the entry wound in all cases of suspected open-globe injuries. In negative Seidel’s test cases, signs such as corneal edema, subconjunctival hemorrhage, or an iris hole may suggest an entry wound (see Image. Subconjunctival Hemorrhage). Apart from the clinical features usually seen in a case of suspected IOFB following penetrating trauma, there are certain signs specific to siderosis bulbi. A slit-lamp examination may reveal rust-colored or yellowish pigment deposits within the corneal stroma or endothelium.[2] Iron deposition within the layers of the iris, particularly stroma and epithelium, results in greenish-brown discoloration, which is reversible in eliminating the foreign body. It is an early sign of ocular siderosis.[17][18]
The pupillary examination may reveal a fixed, dilated pupil, the earliest sign of siderosis bulbi. An exaggerated pupillary constriction to a 0.1% (low-dose) pilocarpine concentration is seen due to denervation hypersensitivity.[19] Evidence of iron deposits within the sphincter and dilator muscles of the iris is seen in histopathology. Both iris discoloration and iron mydriasis are reversible phenomena.[19][20][21] Secondary open-angle glaucoma may develop due to iron deposition in the trabecular meshwork. Eventually, trabecular fibrosclerosis may result due to iron toxicity, resulting in medically uncontrollable glaucoma. The incidence of glaucoma is, however, uncommon in siderosis bulbi (5%).[1][11][22] To rule out a foreign body at the iridocorneal angle, it is critical to perform a gonioscopy in every case of suspected IOFB.[22] Intra-lenticular foreign bodies constitute 10% of all IOFBs and are mostly associated with cataract formation.[23] Classical dark-brown anterior subcapsular deposits may be noted. The mechanism of cataract development is either due to iron deposition or direct trauma to the lens. Progression of ocular siderosis in the case of a localized intra-lenticular foreign body is slower when compared to a posterior-segment foreign body.[24][25]
Siderosis bulbi classically affects the RPE, resulting in pigmentary degeneration of the retina. Iron toxicity may also lead to optic disc edema, though it may resolve after the removal of IOFB.[23] IOFB within the posterior segment may result in vitreous hemorrhage (46%), retinal detachment (RD) (27%), Proliferative vitreoretinopathy (PVR) changes (21% to 89%), the formation of epiretinal membrane, and macular edema. The occurrence of subretinal hemorrhage may further damage the choroid and the inner surface of the sclera.[26][27][28][29][28][27] Infrequently, ocular siderosis may manifest as anterior uveitis, posterior uveitis, or even pan-uveitis.[30][31][28][31]
Evaluation
Radiological evaluation to detect an IOFB plays a key role in the management of ocular trauma. Several useful imaging modalities include X-ray, computed tomography (CT), magnetic resonance imaging (MRI), ultrasonography (USG), ultrasound biomicroscopy (UBM), and Optic coherence tomography (OCT). Electrophysiological tests like Electroretinography (ERG) are essential in assessing retinal damage in ocular siderosis. Ancillary tests, including electrooculogram, fluorescein angiography, and visual field tests, help assess further damage.[32]
Metallic IOFBs are recognized on plain X-ray films as radio-opaque bodies. However, it poses a great challenge in localizing and predicting the nature of foreign bodies and, therefore, has a limited role as a diagnostic modality.[33]
USG, a popular imaging modality, can detect metallic and non-metallic IOFBs. On the B-scan, IOFB appears as a hyperechoic lesion with acoustic back-shadowing.[13] It is a highly sensitive and specific investigation to identify associated ocular injuries, such as lens dislocation, vitreous hemorrhage, RD, and choroidal detachment, even in the presence of media opacities owing to trauma.[34] However, USG has certain limitations. Firstly, it tends to overestimate the size of the foreign body.[35] Secondly, a foreign body lying in the posterior third of the orbit or within the peri-orbital soft tissues may be missed on USG.[34][36] Thirdly, USG requires expertise and is largely operator-dependent. Lastly, it should always be used cautiously in cases of open-globe injuries.[37]
Non-contrast CT (NCCT) is the gold standard investigation for identifying metallic foreign bodies (see Image. It is highly accurate in predicting the nature, location (intraocular, extraocular, or retro-bulbar), and foreign body size. Thin scans (1.0 to 1.5 mm) are preferred for higher resolution. It has a high sensitivity for detecting IOFBs (45% to 65% ≤ 0.06 mm and 100% >0.06 mm size), which may otherwise be missed on the orbital X-ray.[33][38][39][40]
MRI has better sensitivity (95%) than CT scan to detect non-metallic IOFBs and visualize optic nerve, orbital apex, and soft tissue details without radiation exposure.[41] However, MRI is contraindicated in suspected ferromagnetic foreign bodies since these tend to move within the electromagnetic field, causing more ocular damage.[42]
Ultrasound biomicroscopy (UBM) is the preferred imaging for foreign bodies located anteriorly (subconjunctival space, corneal layers, angle, anterior iris surface, ciliary body, pars plana, 100um from the retina). Since UBM requires contact, it should be avoided in cases of an open-globe injury due to an increased risk of intraocular infection.[43][44][45]
Anterior segment OCT (AS-OCT), a non-contact, non-invasive imaging investigation, facilitates the visualization of the anterior segment foreign bodies. Unlike UBM, it ensures greater patient comfort and better compliance. It can also be used as an effective prognosticating tool in ocular siderosis. Owing to its poor penetration across the posterior pigmented layer of the iris, foreign bodies lying behind this plane may often be missed.[46][47]
Posterior segment OCT is a useful tool for detecting the accurate location of an IOFB lying in the posterior segment (epiretinal, intraretinal, or subretinal) and quantifying cystoid macular edema. It can also identify the encapsulation of the foreign body, a factor that helps decide the surgical intervention's timing.[48]
Full-field ERG (ffERG) is the gold standard electrophysiological test for identifying subclinical siderosis bulbi. It is an efficient diagnostic and prognosticating tool in ocular siderosis.[49] In the early phase of the disease, both a- and b-wave amplitude increases (also called the supernormal response).[50][51] The b-wave amplitude subsequently decreases with a reduction in the b /a-wave ratio to less than 1. In advanced cases, an extinguished response is seen on ERG with absent a- and b-waves.[52][11] Early predictors of siderosis bulbi on ERG include the increased amplitude of b-wave (Supernormal response), reduction in the amplitude of Oscillatory potentials, decrease in amplitude of P1 and N1 waves along with a delay in P1-implicit time on mfERG even in the presence of a normal ffERG.[53][54][55] Early removal of the foreign body leads to recovery of ERG amplitudes, as iron toxicity is reversible in the early phase of the disease.[51][56]
Fluorescein angiography in ocular siderosis may reveal hyperfluorescent window defects owing to RPE changes, capillary non-perfusion areas, and ischemic maculopathy.[32][16] Progressive visual field constriction has also been reported in cases of ocular siderosis. Although there may be associated glaucomatous damage, the underlying postulated mechanism involves the insufficiency of retinal circulation in advanced cases.[32][22]
Treatment / Management
Acute presentation following trauma with a metallic foreign body mandates evaluating the patient’s vaccination status and administering the tetanus booster dose accordingly. Systemic and topical broad-spectrum antibiotics should be instituted against the most common organisms, such as gram-positive cocci (streptococcus, coagulase-negative staphylococcus), anaerobic bacteria (clostridium species), and gram-negative bacilli (Escherichia coli, Klebsiella pneumoniae).[57] Once the metallic foreign body has been identified on imaging, it is strongly recommended that the foreign body be promptly removed to avoid the occurrence of siderosis bulbi (in case of an iron IOFB) and endophthalmitis. A single-setting surgical procedure is usually associated with better visual outcomes when compared to multiple surgeries.[58](B2)
The indications for immediate removal include foreign body localized in the anterior chamber, vitreous cavity, and a non-encapsulated foreign body in the retina.[59][52] Surgical removal becomes cumbersome once the foreign body in the posterior segment is encapsulated.[52] It is also important to emphasize that delayed surgery (for more than 14 days) is associated with an increased risk of tractional RD and PVR changes.[60] The intra-lenticular iron foreign body may be removed simultaneously with cataractous lens extraction. Iron particles tend to leak out, especially in the periphery, further predisposing to siderosis bulbi.[59] Immediate wound closure must be performed in all cases of open-globe injuries. However, the surgical removal of IOFBs can be delayed due to the non-availability of the vitreoretinal setup or in cases where corneal edema precludes Pars Plana Vitrectomy (PPV).[57] The ultimate decision to remove an IOFB must be weighed against the risk-benefit ratio.(B3)
In cases of delayed surgical intervention, it is critical to perform serial assessments with ERG testing every 2 to 3 months. If the ERG remains stable, the patient can be observed further with gradually increasing intervals between subsequent follow-ups. On every follow-up, best-corrected visual acuity, ophthalmoscopy, appropriate imaging, and serial ERG should be evaluated. If the patient appears non-compliant to follow-up or a diminishing response on ERG is noted, immediate removal is warranted.[52](B3)
Surgical Management
Posterior segment metallic IOFB may be removed via the traditional external approach using an external electromagnet (EEM) or an internal approach using forceps or intra-ocular magnets (IOMs).[11] In the external approach, a sclerotomy is made at 4.5mm from the limbus, and extraction is initiated using EEM under visualization of the indirect ophthalmoscope.[61] This approach is associated with a higher incidence of iatrogenic ocular injuries, such as hyphema, vitreous hemorrhage, retinal laceration, RD, vitreous prolapse, trauma to the iris, lens, and zonules. Thus, using EEM is now obsolete and only reserved for removing IOFB remnants.[62][61](B2)
In the internal approach, 23G or 25G (sutureless) PPV is done using forceps or an IOM.[63] 20-gauge vitrectomy may be indicated in cases of large foreign bodies.[57] Forceps are advisable over IOMs as removing the metallic foreign body may be difficult once the IOMs or the IOFBs lose their magnetic properties.[11] This approach is comparatively less traumatic than the external approach. Surgical removal of IOFB and the resultant intra-operative complications can be concurrently managed using this approach.[62] It is recommended to use perfluorocarbon liquid (PFCL) before lifting the IOFB to prevent macular damage.[61] A new surgical procedure, the handshake technique, has been recently described wherein 2 IOMs are introduced through the PPV sclerotomies followed by safe delivery of the IOFB through the corneoscleral tunnel. This technique is especially preferred for large foreign bodies as it doesn’t require enlargement of the pre-existing sclerotomy.[64](B2)
For foreign bodies in the anterior segment, removal is initiated through the limbal approach in cases of foreign bodies larger than 6mm or through the sclera for smaller foreign bodies.[65] Removal through the entry wound is usually not advocated, except in cases of a large foreign body or a gaping corneal wound, due to the risk of scarring and endothelial damage.[39] Balanced salt solution or ophthalmic viscoelastic devices may dislodge a foreign body in the anterior chamber. Gonioscopy-assisted removal is warranted for foreign bodies located in the irideocorneal angle.[39] IOFBs within the iris may be removed by iridotomy or iridectomy.[66] (B3)
Role of Deferoxamine
Deferoxamine is a chelating agent with a high affinity for free iron ions. It is used in thalassaemic patients undergoing multiple blood transfusions to avoid siderosis due to iron overload.[67] Subconjunctival use of deferoxamine (10 to 100 mg) has been shown to prevent the development of ocular siderosis. In advanced siderosis, where cells are already damaged, deferoxamine cannot reverse the toxic effects of iron as it cannot remove the bound iron ions from the tissue.[68] Deferoxamine-related toxicity, such as bone dysplasia, sensorineural hearing loss, nyctalopia, color vision impairment, RPE alteration, and reduction in ERG amplitudes, limits its use in the management of ocular siderosis.[69](B2)
Differential Diagnosis
Since retinal arteriolar narrowing and sheathing with pigmentary retinal degeneration can be seen in siderosis bulbi, it closely resembles retinitis pigmentosa (RP). In rare cases of suspected unilateral RP, the diagnosis clinches more towards ocular siderosis when associated with a typical history of trauma with an iron foreign body.[70][13][70] Mydriasis, with a hypersensitive response to 0.1% pilocarpine in ocular siderosis, mimics Adie’s tonic pupil and must be considered 1 of the differential diagnoses. The pathophysiology of Adie’s tonic pupil involves damage to the ciliary ganglion, as opposed to the local parasympathetic neuropathy in siderosis bulbi.[20][23][71]
Prognosis
Factors such as young age, large IOFBs (mean length= 5.7mm) with high kinetic energy, best-corrected visual acuity < 20/200 at presentation, prolonged retention of foreign body, posterior segment IOFBs, and associated hyphema, vitreous hemorrhage, RD or endophthalmitis at presentation are associated with a poorer prognosis.[72][73][74][75] Multiple surgeries are associated with enhanced morbidity. Ocular trauma score (OTS), developed by Kuhn et al., can be used to prognosticate ocular siderosis and predict visual outcomes in penetrating ocular injuries.[76][6] The length of the entry wound also determines the risk of retinal damage. Less energy dissipation occurs in shorter wounds, allowing deeper eye penetration and significant retinal damage.[66] Blunt IOFBs tend to cause more damage to the globe than the sharper ones of the same size, owing to significant energy transfer at the time of impact.[77]
Complications
IOFB can lead to several complications, such as those associated with an open-globe injury. Endophthalmitis is the most dreaded complication following ocular trauma. Post-traumatic endophthalmitis has been reported to develop in 2.1% to 11.9% of patients with open-globe injury in the absence of IOFB. In contrast, endophthalmitis associated with an IOFB accounts for 3.8% to 48.1% of cases.[78][79][80] Poor prognosticating factors include increased occurrence of virulent organisms, associated tissue damage, and delay in management.[81] Another sight-threatening complication of an open-globe injury is Sympathetic Ophthalmia (SO). It is a bilateral granulomatous pan-uveitis usually following penetrating ocular trauma or surgery. The incidence of SO is reported as 0.28-1.9% in penetrating ocular trauma.[82][83][84] IOFB can also be associated with several anterior segment complications, such as hyphema, traumatic cataracts, capsular rupture, subluxation or dislocation, and secondary open-angle glaucoma.[75][6][1][25] Siderosis bulbi can also lead to optic atrophy and cystoid macular edema.[85][32] There is also an increased risk of epiretinal membrane formation, leading to macular puckering, PVR, and retinal detachment.[26][27]
Deterrence and Patient Education
Public awareness regarding workplace-related ocular trauma should be strengthened as prevention is the key to avoiding the dreaded complications of penetrating ocular injuries and siderosis bulbi. A better understanding of the detrimental consequences of ocular siderosis encourages people to take appropriate measures for eye protection at workplaces, such as safety glasses, eye goggles, and face shields. Patients must be warned about the complications of open-globe trauma and siderosis bulbi. They must be counseled regarding the final prognosis and the importance of regular follow-up visits.
Pearls and Other Issues
A thorough history and meticulous examination are recommended in every case of ocular trauma to rule out the intraocular foreign body. Radiological investigations play an instrumental role in timely detection and appropriate management. Serial monitoring and regular follow-up are advocated in all cases of suspected ocular siderosis.
Enhancing Healthcare Team Outcomes
A general ophthalmologist must be well-trained in dealing with cases of ocular trauma. A high index of suspicion for the presence of an intraocular foreign body must be maintained in all cases of ocular injuries, especially in young children who may present without any apparent history of trauma. In cases where a vitreoretinal facility is unavailable, a proficient specialist must be consulted immediately.
Media
(Click Image to Enlarge)

Subconjunctival Hemorrhage. The image is a subconjunctival hemorrhage with evidence of an entry wound (blue arrow) in a 29-year-old male following a hammer and chisel injury.
Contributed by I Acharya, MBBS
(Click Image to Enlarge)
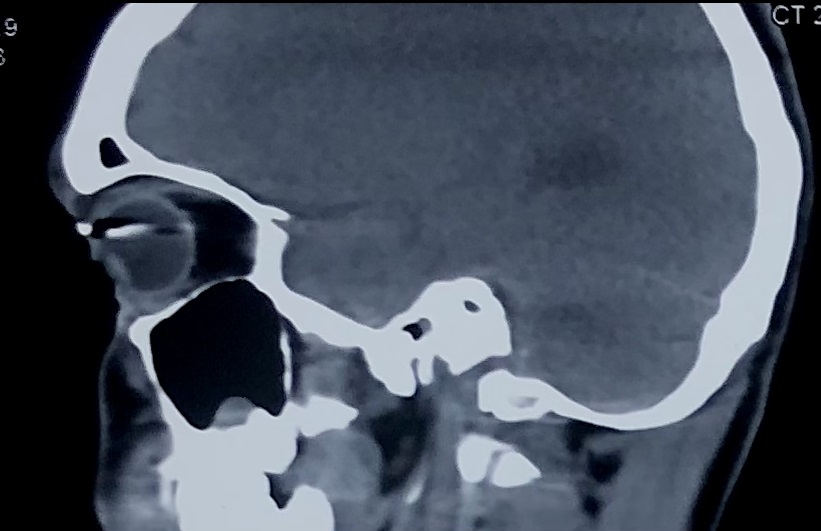
Intraocular Foreign Body Following a Penetrating Injury. NCCT, sagittal view, showing hyperdense lesion suggestive of an IOFB following a penetrating injury
Contributed by A Agarwal, MBBS
References
BALLANTYNE JF. Siderosis bulbi. The British journal of ophthalmology. 1954 Dec:38(12):727-33 [PubMed PMID: 13219251]
Talamo JH, Topping TM, Maumenee AE, Green WR. Ultrastructural studies of cornea, iris and lens in a case of siderosis bulbi. Ophthalmology. 1985 Dec:92(12):1675-80 [PubMed PMID: 4088618]
Level 3 (low-level) evidenceJonas JB, Knorr HL, Budde WM. Prognostic factors in ocular injuries caused by intraocular or retrobulbar foreign bodies. Ophthalmology. 2000 May:107(5):823-8 [PubMed PMID: 10811069]
Level 2 (mid-level) evidenceGreven CM,Engelbrecht NE,Slusher MM,Nagy SS, Intraocular foreign bodies: management, prognostic factors, and visual outcomes. Ophthalmology. 2000 Mar; [PubMed PMID: 10711903]
Level 2 (mid-level) evidenceKong Y, Tang X, Kong B, Jiang H, Chen Y. Six-year clinical study of firework-related eye injuries in North China. Postgraduate medical journal. 2015 Jan:91(1071):26-9. doi: 10.1136/postgradmedj-2014-132837. Epub [PubMed PMID: 25583736]
Level 2 (mid-level) evidenceZhu L, Shen P, Lu H, Du C, Shen J, Gu Y. Ocular Trauma Score in Siderosis Bulbi With Retained Intraocular Foreign Body. Medicine. 2015 Sep:94(39):e1533. doi: 10.1097/MD.0000000000001533. Epub [PubMed PMID: 26426616]
Wu TT, Kung YH, Sheu SJ, Yang CA. Lens siderosis resulting from a tiny missed intralenticular foreign body. Journal of the Chinese Medical Association : JCMA. 2009 Jan:72(1):42-4. doi: 10.1016/S1726-4901(09)70019-X. Epub [PubMed PMID: 19181597]
Level 3 (low-level) evidenceDemircan N, Soylu M, Yagmur M, Akkaya H, Ozcan AA, Varinli I. Pars plana vitrectomy in ocular injury with intraocular foreign body. The Journal of trauma. 2005 Nov:59(5):1216-8 [PubMed PMID: 16385302]
Level 2 (mid-level) evidenceWilliams DF, Mieler WF, Abrams GW, Lewis H. Results and prognostic factors in penetrating ocular injuries with retained intraocular foreign bodies. Ophthalmology. 1988 Jul:95(7):911-6 [PubMed PMID: 3262852]
Khani SC, Mukai S. Posterior segment intraocular foreign bodies. International ophthalmology clinics. 1995 Winter:35(1):151-61 [PubMed PMID: 7751127]
Kannan NB, Adenuga OO, Rajan RP, Ramasamy K. Management of Ocular Siderosis: Visual Outcome and Electroretinographic Changes. Journal of ophthalmology. 2016:2016():7272465. doi: 10.1155/2016/7272465. Epub 2016 Mar 17 [PubMed PMID: 27073692]
Chao HM, Chen YH, Liu JH, Lee SM, Lee FL, Chang Y, Yeh PH, Pan WH, Chi CW, Liu TY, Lui WY, Ho LT, Kuo CD, Lin DE, Chan CC, Yang DM, Lin AM, Chao FP. Iron-generated hydroxyl radicals kill retinal cells in vivo: effect of ferulic acid. Human & experimental toxicology. 2008 Apr:27(4):327-39. doi: 10.1177/0960327108092294. Epub [PubMed PMID: 18684804]
Level 3 (low-level) evidenceCasini G, Sartini F, Loiudice P, Benini G, Menchini M. Ocular siderosis: a misdiagnosed cause of visual loss due to ferrous intraocular foreign bodies-epidemiology, pathogenesis, clinical signs, imaging and available treatment options. Documenta ophthalmologica. Advances in ophthalmology. 2021 Apr:142(2):133-152. doi: 10.1007/s10633-020-09792-x. Epub 2020 Sep 19 [PubMed PMID: 32949328]
Level 3 (low-level) evidenceMasciulli L, Anderson DR, Charles S. Experimental ocular siderosis in the squirrel monkey. American journal of ophthalmology. 1972 Oct:74(4):638-61 [PubMed PMID: 4116414]
Level 3 (low-level) evidenceCIBIS PA, YAMASHITA T. Experimental aspects of ocular siderosis and hemosiderosis. American journal of ophthalmology. 1959 Nov:48(5)Pt2():465-80 [PubMed PMID: 13810275]
Shaikh S, Blumenkranz MS. Fluorescein angiographic findings in ocular siderosis. American journal of ophthalmology. 2001 Jan:131(1):136-8 [PubMed PMID: 11162994]
Level 3 (low-level) evidenceWelch RB. Two remarkable events in the field of intraocular foreign body: (1) The reversal of siderosis bulbi. (2) The spontaneous extrusion of an intraocular copper foreign body. Transactions of the American Ophthalmological Society. 1975:73():187-203 [PubMed PMID: 1108372]
Level 3 (low-level) evidenceBarr CC, Vine AK, Martonyi CL. Unexplained heterochromia. Intraocular foreign body demonstrated by computed tomography. Survey of ophthalmology. 1984 Mar-Apr:28(5):409-11 [PubMed PMID: 6719337]
Level 3 (low-level) evidenceVerhoeff FH, SIDEROSIS BULBI. The British journal of ophthalmology. 1918 Nov [PubMed PMID: 18167834]
Monteiro ML, Ulrich RF, Imes RK, Fung WE, Hoyt WF. Iron mydriasis. American journal of ophthalmology. 1984 Jun:97(6):794-6 [PubMed PMID: 6731551]
Level 3 (low-level) evidenceBlack NM. Siderosis Bulbi with Dilated Inactive Pupil. Recovery of Pupillary Activity After Removal of Foreign Body. Transactions of the American Ophthalmological Society. 1923:21():171-82 [PubMed PMID: 16692633]
Kearns M, McDonald R. Generalised siderosis from an iris foreign body. Australian journal of ophthalmology. 1980 Nov:8(4):311-3 [PubMed PMID: 7224987]
Level 3 (low-level) evidenceHope-Ross M,Mahon GJ,Johnston PB, Ocular siderosis. Eye (London, England). 1993 [PubMed PMID: 8224298]
RYCHENER RO. Siderosis following intralenticular foreign body. American journal of ophthalmology. 1946 Mar:29():346 [PubMed PMID: 21066075]
Siantar RG, Agrawal R, Heng LW, Ho BC. Histopathologically proven siderotic cataract with disintegrated intralenticular foreign body. Indian journal of ophthalmology. 2013 Jan-Feb:61(1):30-2. doi: 10.4103/0301-4738.105051. Epub [PubMed PMID: 23275219]
Level 3 (low-level) evidenceKuhn F, Kovacs B. Management of postequatorial magnetic intraretinal foreign bodies. International ophthalmology. 1989 Sep:13(5):321-5 [PubMed PMID: 2625380]
Slusher MM,Sarin LK,Federman JL, Management of intraretinal foreign bodies. Ophthalmology. 1982 Apr; [PubMed PMID: 7099555]
Percival SP. Late complications from posterior segment intraocular foreign bodies with particular reference to retinal detachment. The British journal of ophthalmology. 1972 Jun:56(6):462-8 [PubMed PMID: 5069185]
Colyer MH, Weber ED, Weichel ED, Dick JS, Bower KS, Ward TP, Haller JA. Delayed intraocular foreign body removal without endophthalmitis during Operations Iraqi Freedom and Enduring Freedom. Ophthalmology. 2007 Aug:114(8):1439-47 [PubMed PMID: 17331579]
Level 2 (mid-level) evidencePolitis M, Rosin B, Amer R. Ocular Siderosis Subsequent to a Missed Pars Plana Metallic Foreign Body that Masqueraded as Refractory Intermediate Uveitis. Ocular immunology and inflammation. 2018:26(4):598-600. doi: 10.1080/09273948.2016.1240206. Epub 2016 Nov 16 [PubMed PMID: 27849408]
Yeh S, Ralle M, Phan IT, Francis PJ, Rosenbaum JT, Flaxel CJ. Occult intraocular foreign body masquerading as panuveitis: inductively coupled mass spectrometry and electrophysiologic analysis. Journal of ophthalmic inflammation and infection. 2012 Jun:2(2):99-103. doi: 10.1007/s12348-011-0035-9. Epub 2011 Jul 31 [PubMed PMID: 21805383]
Schocket SS, Lakhanpal V, Varma SD. Siderosis from a retained intraocular stone. Retina (Philadelphia, Pa.). 1981:1(3):201-7 [PubMed PMID: 7348836]
Level 3 (low-level) evidenceSaeed A, Cassidy L, Malone DE, Beatty S. Plain X-ray and computed tomography of the orbit in cases and suspected cases of intraocular foreign body. Eye (London, England). 2008 Nov:22(11):1373-7 [PubMed PMID: 17558386]
Level 2 (mid-level) evidenceMcNicholas MM, Brophy DP, Power WJ, Griffin JF. Ocular trauma: evaluation with US. Radiology. 1995 May:195(2):423-7 [PubMed PMID: 7724761]
Cascone G, Filippello M, Ferri R, Scimone G, Zagami A. B-scan echographic measurement of endobulbar foreign bodies. Ophthalmologica. Journal international d'ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 1994:208(4):192-4 [PubMed PMID: 7970544]
Level 3 (low-level) evidenceWeisman RA, Savino PJ, Schut L, Schatz NJ. Computed tomography in penetrating wounds of the orbit with retained foreign bodies. Archives of otolaryngology (Chicago, Ill. : 1960). 1983 Apr:109(4):265-8 [PubMed PMID: 6830522]
Level 3 (low-level) evidenceWang K, Liu J, Chen M. Role of B-scan ultrasonography in the localization of intraocular foreign bodies in the anterior segment: a report of three cases. BMC ophthalmology. 2015 Aug 14:15():102. doi: 10.1186/s12886-015-0076-1. Epub 2015 Aug 14 [PubMed PMID: 26268356]
Level 3 (low-level) evidenceChacko JG, Figueroa RE, Johnson MH, Marcus DM, Brooks SE. Detection and localization of steel intraocular foreign bodies using computed tomography. A comparison of helical and conventional axial scanning. Ophthalmology. 1997 Feb:104(2):319-23 [PubMed PMID: 9052639]
Lit ES, Young LH. Anterior and posterior segment intraocular foreign bodies. International ophthalmology clinics. 2002 Summer:42(3):107-20 [PubMed PMID: 12131588]
Otto PM, Otto RA, Virapongse C, Friedman SM, Emerson S, Li KC, Malot R, Kaude JV, Staab EV. Screening test for detection of metallic foreign objects in the orbit before magnetic resonance imaging. Investigative radiology. 1992 Apr:27(4):308-11 [PubMed PMID: 1601622]
Weber AL, Caruso P, Sabates NR. The optic nerve: radiologic, clinical, and pathologic evaluation. Neuroimaging clinics of North America. 2005 Feb:15(1):175-201 [PubMed PMID: 15927867]
Ta CN, Bowman RW. Hyphema caused by a metallic intraocular foreign body during magnetic resonance imaging. American journal of ophthalmology. 2000 Apr:129(4):533-4 [PubMed PMID: 10764867]
Level 3 (low-level) evidenceLaroche D, Ishikawa H, Greenfield D, Liebmann JM, Ritch R. Ultrasound biomicroscopic localization and evaluation of intraocular foreign bodies. Acta ophthalmologica Scandinavica. 1998 Aug:76(4):491-5 [PubMed PMID: 9716340]
Level 3 (low-level) evidenceSangermani C, Mora P, Mancini C, Vecchi M, Gandolfi SA. Ultrasound biomicroscopy in two cases of ocular siderosis with secondary glaucoma. Acta ophthalmologica. 2010 Feb:88(1):e1-2. doi: 10.1111/j.1755-3768.2009.01521.x. Epub 2009 Jun 26 [PubMed PMID: 19563373]
Level 3 (low-level) evidenceBarash D, Goldenberg-Cohen N, Tzadok D, Lifshitz T, Yassur Y, Weinberger D. Ultrasound biomicroscopic detection of anterior ocular segment foreign body after trauma. American journal of ophthalmology. 1998 Aug:126(2):197-202 [PubMed PMID: 9727513]
Level 3 (low-level) evidenceMansouri K, Sommerhalder J, Shaarawy T. Prospective comparison of ultrasound biomicroscopy and anterior segment optical coherence tomography for evaluation of anterior chamber dimensions in European eyes with primary angle closure. Eye (London, England). 2010 Feb:24(2):233-9. doi: 10.1038/eye.2009.103. Epub 2009 May 15 [PubMed PMID: 19444291]
Level 2 (mid-level) evidenceWylegala E, Dobrowolski D, Nowińska A, Tarnawska D. Anterior segment optical coherence tomography in eye injuries. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2009 Apr:247(4):451-5. doi: 10.1007/s00417-008-0937-x. Epub 2008 Sep 3 [PubMed PMID: 18766361]
Level 2 (mid-level) evidenceChao HM, Chen SJ, Hsu WM, Lee FL, Chen KH. Siderosis oculi: visual dysfunctions even after iron removal: a role of OCT. Cutaneous and ocular toxicology. 2006:25(2):131-40 [PubMed PMID: 16835148]
Level 3 (low-level) evidenceKARPE G. Early diagnosis of siderosis retina by the use of electroretinography. Documenta ophthalmologica. Advances in ophthalmology. 1948:2(1 vol.):277-96 [PubMed PMID: 18121442]
Level 3 (low-level) evidenceDeclercq SS, Meredith PC, Rosenthal AR. Experimental siderosis in the rabbit: correlation between electroretinography and histopathology. Archives of ophthalmology (Chicago, Ill. : 1960). 1977 Jun:95(6):1051-8 [PubMed PMID: 869748]
Level 3 (low-level) evidenceImaizumi M, Matsumoto CS, Yamada K, Nanba Y, Takaki Y, Nakatsuka K. Electroretinographic assessment of early changes in ocular siderosis. Ophthalmologica. Journal international d'ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 2000 Sep-Oct:214(5):354-9 [PubMed PMID: 10965251]
Level 3 (low-level) evidenceSneed SR, Weingeist TA. Management of siderosis bulbi due to a retained iron-containing intraocular foreign body. Ophthalmology. 1990 Mar:97(3):375-9 [PubMed PMID: 2336277]
Level 3 (low-level) evidenceTanabe J, Shirao Y, Oda N, Kawasaki K. Evaluation of retinal integrity in eyes with retained intraocular metallic foreign body by ERG and EOG. Documenta ophthalmologica. Advances in ophthalmology. 1992:79(1):71-8 [PubMed PMID: 1568423]
Level 3 (low-level) evidenceGupta S, Midha N, Gogia V, Sahay P, Pandey V, Venkatesh P. Sensitivity of multifocal electroretinography (mfERG) in detecting siderosis. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2015 Dec:50(6):485-90. doi: 10.1016/j.jcjo.2015.08.011. Epub [PubMed PMID: 26651311]
Sahay P, Kumawat D, Gupta S, Tripathy K, Vohra R, Chandra M, Venkatesh P. Detection and monitoring of subclinical ocular siderosis using multifocal electroretinogram. Eye (London, England). 2019 Oct:33(10):1547-1555. doi: 10.1038/s41433-019-0442-y. Epub 2019 Apr 24 [PubMed PMID: 31019264]
Kuhn F, Witherspoon CD, Skalka H, Morris R. Improvement of siderotic ERG. European journal of ophthalmology. 1992 Jan-Mar:2(1):44-5 [PubMed PMID: 1638168]
Level 3 (low-level) evidenceYeh S, Colyer MH, Weichel ED. Current trends in the management of intraocular foreign bodies. Current opinion in ophthalmology. 2008 May:19(3):225-33. doi: 10.1097/ICU.0b013e3282fa75f1. Epub [PubMed PMID: 18408498]
Level 3 (low-level) evidenceFalavarjani KG, Hashemi M, Modarres M, Parvaresh MM, Naseripour M, Nazari H, Fazel AJ. Vitrectomy for posterior segment intraocular foreign bodies, visual and anatomical outcomes. Middle East African journal of ophthalmology. 2013 Jul-Sep:20(3):244-7. doi: 10.4103/0974-9233.114803. Epub [PubMed PMID: 24014990]
Level 2 (mid-level) evidenceFoss AJ, Forbes JE, Morgan J. An intralenticular foreign body and a clear lens. The British journal of ophthalmology. 1993 Dec:77(12):828 [PubMed PMID: 8110688]
Level 3 (low-level) evidenceCleary PE, Ryan SJ. Vitrectomy in penetrating eye injury. Results of a controlled trial of vitrectomy in an experimental posterior penetrating eye injury in the rhesus monkey. Archives of ophthalmology (Chicago, Ill. : 1960). 1981 Feb:99(2):287-92 [PubMed PMID: 7469867]
Level 3 (low-level) evidenceGuevara-Villarreal DA, Rodríguez-Valdés PJ. Posterior Segment Intraocular Foreign Body: Extraction Surgical Techniques, Timing, and Indications for Vitrectomy. Journal of ophthalmology. 2016:2016():2034509. doi: 10.1155/2016/2034509. Epub 2016 Nov 29 [PubMed PMID: 28025619]
Mester V, Kuhn F. Ferrous intraocular foreign bodies retained in the posterior segment: management options and results. International ophthalmology. 1998:22(6):355-62 [PubMed PMID: 10937851]
Level 2 (mid-level) evidenceSingh R, Bhalekar S, Dogra MR, Gupta A. 23-gauge vitrectomy with intraocular foreign body removal via the limbus: an alternative approach for select cases. Indian journal of ophthalmology. 2014 Jun:62(6):707-10. doi: 10.4103/0301-4738.116458. Epub [PubMed PMID: 24008799]
Level 3 (low-level) evidenceDhoble P, Khodifad A. Combined Cataract Extraction With Pars Plana Vitrectomy and Metallic Intraocular Foreign Body Removal Through Sclerocorneal Tunnel Using a Novel "Magnet Handshake" Technique. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2018 Mar-Apr:7(2):114-118. doi: 10.22608/APO.2017207. Epub 2017 Sep 4 [PubMed PMID: 28868832]
Yuksel K, Celik U, Alagoz C, Dundar H, Celik B, Yazıcı AT. 23 gauge pars plana vitrectomy for the removal of retained intraocular foreign bodies. BMC ophthalmology. 2015 Jul 16:15():75. doi: 10.1186/s12886-015-0067-2. Epub 2015 Jul 16 [PubMed PMID: 26178019]
Loporchio D, Mukkamala L, Gorukanti K, Zarbin M, Langer P, Bhagat N. Intraocular foreign bodies: A review. Survey of ophthalmology. 2016 Sep-Oct:61(5):582-96. doi: 10.1016/j.survophthal.2016.03.005. Epub 2016 Mar 17 [PubMed PMID: 26994871]
Level 3 (low-level) evidenceKwiatkowski JL. Current recommendations for chelation for transfusion-dependent thalassemia. Annals of the New York Academy of Sciences. 2016 Mar:1368(1):107-14. doi: 10.1111/nyas.13088. Epub [PubMed PMID: 27186943]
Wise JB. Treatment of experimental siderosis bulbi, vitreous hemorrhage, and corneal blood staining with deferoxamine. Archives of ophthalmology (Chicago, Ill. : 1960). 1966 May:75(5):698-707 [PubMed PMID: 5937181]
Level 3 (low-level) evidenceBaath JS, Lam WC, Kirby M, Chun A. Deferoxamine-related ocular toxicity: incidence and outcome in a pediatric population. Retina (Philadelphia, Pa.). 2008 Jun:28(6):894-9. doi: 10.1097/IAE.0b013e3181679f67. Epub [PubMed PMID: 18536609]
Level 2 (mid-level) evidenceTemkar S, Mukhija R, Venkatesh P, Chawla R. Pseudo retinitis pigmentosa in a case of missed intraocular foreign body. BMJ case reports. 2017 Jul 31:2017():. pii: bcr-2017-220385. doi: 10.1136/bcr-2017-220385. Epub 2017 Jul 31 [PubMed PMID: 28765492]
Level 3 (low-level) evidenceWilhelm H. Neuro-ophthalmology of pupillary function--practical guidelines. Journal of neurology. 1998 Sep:245(9):573-83 [PubMed PMID: 9758294]
Szijártó Z, Gaál V, Kovács B, Kuhn F. Prognosis of penetrating eye injuries with posterior segment intraocular foreign body. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2008 Jan:246(1):161-5 [PubMed PMID: 17674019]
Level 2 (mid-level) evidenceWickham L, Xing W, Bunce C, Sullivan P. Outcomes of surgery for posterior segment intraocular foreign bodies--a retrospective review of 17 years of clinical experience. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2006 Dec:244(12):1620-6 [PubMed PMID: 16788826]
Level 2 (mid-level) evidenceEhlers JP, Kunimoto DY, Ittoop S, Maguire JI, Ho AC, Regillo CD. Metallic intraocular foreign bodies: characteristics, interventions, and prognostic factors for visual outcome and globe survival. American journal of ophthalmology. 2008 Sep:146(3):427-433. doi: 10.1016/j.ajo.2008.05.021. Epub 2008 Jul 9 [PubMed PMID: 18614135]
Level 2 (mid-level) evidenceZhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in china: clinical characteristics, prognostic factors, and visual outcomes in 1,421 eyes. American journal of ophthalmology. 2011 Jul:152(1):66-73.e1. doi: 10.1016/j.ajo.2011.01.014. Epub 2011 May 6 [PubMed PMID: 21529762]
Level 2 (mid-level) evidenceKuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The Ocular Trauma Score (OTS). Ophthalmology clinics of North America. 2002 Jun:15(2):163-5, vi [PubMed PMID: 12229231]
Potts AM, Distler JA. Shape factor in the penetration of intraocular foreign bodies. American journal of ophthalmology. 1985 Jul 15:100(1):183-7 [PubMed PMID: 4014371]
Level 3 (low-level) evidenceDehghani AR, Rezaei L, Salam H, Mohammadi Z, Mahboubi M. Post traumatic endophthalmitis: incidence and risk factors. Global journal of health science. 2014 Jun 30:6(6):68-72. doi: 10.5539/gjhs.v6n6p68. Epub 2014 Jun 30 [PubMed PMID: 25363107]
Level 2 (mid-level) evidenceBoldt HC, Pulido JS, Blodi CF, Folk JC, Weingeist TA. Rural endophthalmitis. Ophthalmology. 1989 Dec:96(12):1722-6 [PubMed PMID: 2622617]
Level 2 (mid-level) evidenceVerbraeken H, Rysselaere M. Post-traumatic endophthalmitis. European journal of ophthalmology. 1994 Jan-Mar:4(1):1-5 [PubMed PMID: 8019116]
Danis RP. Endophthalmitis. Ophthalmology clinics of North America. 2002 Jun:15(2):243-8 [PubMed PMID: 12229241]
Ozbek Z, Arikan G, Yaman A, Oner H, Bajin MS, Saatci AO. Sympathetic ophthalmia following vitreoretinal surgery. International ophthalmology. 2010 Apr:30(2):221-7. doi: 10.1007/s10792-009-9313-z. Epub 2009 Jul 9 [PubMed PMID: 19588077]
Level 3 (low-level) evidenceAlbert DM, Diaz-Rohena R. A historical review of sympathetic ophthalmia and its epidemiology. Survey of ophthalmology. 1989 Jul-Aug:34(1):1-14 [PubMed PMID: 2678549]
Level 2 (mid-level) evidenceLiddy L, Stuart J. Sympathetic ophthalmia in Canada. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 1972 Apr:7(2):157-9 [PubMed PMID: 4274314]
Sandhu HS, Young LH. Ocular siderosis. International ophthalmology clinics. 2013 Fall:53(4):177-84. doi: 10.1097/IIO.0b013e3182a5b58f. Epub [PubMed PMID: 24088944]