Introduction
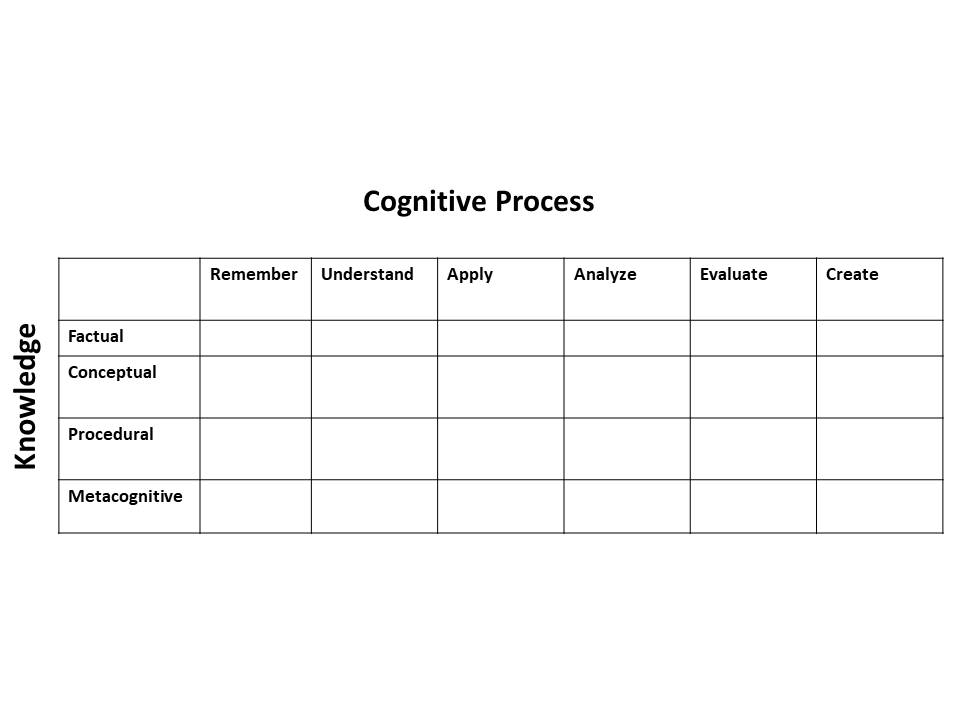
Benjamin Bloom and colleagues developed the Taxonomy of educational objectives: the cognitive domain in 1956, which serves as the foundation for educational objectives and learning goals. Bloom’s taxonomy created a common language such that learning materials could be compared between institutions and provided a way to assess what a curriculum offered within the learning domain. The three learning domains are cognitive, affective, and psychomotor. Bloom’s taxonomy published in 1956 is specific to the cognitive domain and presents a hierarchical structure with six levels of learning: knowledge (lowest level), comprehension, application, analysis, synthesis, and evaluation (highest level). Bloom’s taxonomy was revised in 2001 by Lorin Anderson and David Krathwohl (one of the authors of the original taxonomy). Regarding this revision, Krathwohl commented on how Bloom’s taxonomy went from a unidimensional ladder of cognitive processes to a two-dimensional structure of cognitive processes and types of knowledge. The knowledge dimension consisted of factual knowledge, conceptual knowledge, procedural knowledge, and metacognitive knowledge subtypes. The dimension of cognitive processes resembled the original taxonomy, with six levels: remember, understand, apply, analyze, evaluate, and create. The names of the levels were changed from nouns to verbs, and the highest level became “create.”[1]
Since Bloom’s taxonomy for the cognitive domain, additional taxonomies have been created both for the cognitive domain and for the affective and psychomotor domains. New taxonomies will continue to be designed to fit wider educational needs. One example of another taxonomy is Fink’s Taxonomy of Significant Learning, which consists of six parts: learning how to learn, foundational knowledge, application, integration, human dimension, and caring.[2]
These taxonomies can be useful to help guide the creation of curriculum learning objectives and to reveal what a curriculum might be lacking. Often in medical education, learning objectives focus on knowledge more than the other domains.[3] The field of medical simulation comprises a variety of educational tools and approaches that can reach learning objectives across all three educational domains.