Continuing Education Activity
Peripheral venous access is a key need for resuscitating patients of all ages. An ideal site for venous catheterization is one that is easy to access and poses very little risk to the patient. Sites for venous access in young children include the hands, feet, forearms, and scalp. The most common reasons for intravenous therapy in infants include the delivery of maintenance fluids, blood and blood products, medications, and nutrition. The scalp veins are commonly used to secure intravenous access in neonates and infants, often after unsuccessful attempts at cannulation of upper and lower limb veins. This activity illustrates the technique, indications and contraindications of scalp vein catheterization and highlights the role of the interprofessional team in the management of infants requiring intravenous access.
Objectives:
- Identify the techniques for performing scalp vein catheterization.
- Describe the indications for scalp vein catheterization.
- Outline the complications of scalp vein catheterization.
- Explain the importance of improving care coordination among the interprofessional team to enhance the delivery of care for patients requiring scalp vein catheterization.
Introduction
Peripheral venous access is a hallmark of resuscitation in patients of all ages. Ideal sites for venous catheterization are easy to access and pose the least risk to the patient. Sites for venous access in young children include the hands, feet, forearms, and scalp. The most common reasons for intravenous therapy in infants are to deliver maintenance fluids, blood and blood products, medications, and nutrition. The scalp veins are commonly used to secure access in neonates and infants often after unsuccessful attempts at cannulation of upper and lower limb veins. Scalp veins offer ease of stabilization and ease of access in this age group. Scalp veins in neonates/infants typically have less overlying subcutaneous fat compared to other peripheral sites to allow easier visualization and cannulation.[1][2][3]
Anatomy and Physiology
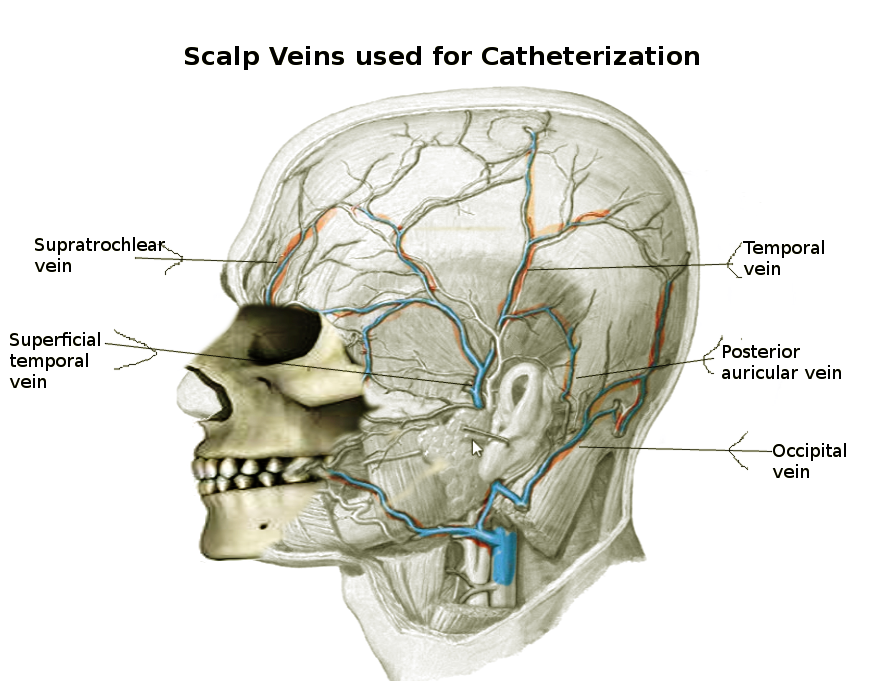
Scalp and facial veins are rather prominent in newborns/infants, are valveless, and are only thinly obscured by fine hair. The most commonly used veins include the superficial temporal, frontal (supratrochlear), occipital, and pre- and post-auricular. The superficial temporal vein drains the entire lateral area of the scalp before passing inferiorly to join in the retromandibular vein's formation and then draining into the external jugular vein. The frontal/supratrochlear vein drains the anterior part of the scalp from the superciliary arches to the vertex, passes into the medial portion of the orbit to join the supraorbital vein in forming the angular vein (linked to cavernous sinus by ophthalmic veins), further draining into the facial and then into the internal jugular vein. The occipital vein drains the posterior aspect of the scalp, pierces the posterior neck musculature and drains either directly into the internal jugular or the internal jugular vein via the posterior auricular. Lastly, the auricular veins run anteriorly and posteriorly to the ear and eventually drain into the external jugular vein.
Indications
Scalp vein cannulation is indicated in young patients requiring administration of intravenous fluids or other medications, where peripheral intravenous access is not possible.
Contraindications
There is a relative contraindication for scalp vein cannulation placement in an older infant as there is a risk of easy dislodgement. Cannulation of scalp vein in areas with superficial skin lesions or evidence of infection should be avoided.
Equipment
- Choose the smallest catheter available (23G, 25G, or 27G butterfly/scalp vein set) in the shortest length (typically 3/4 inch)
- 24G catheter-over-needle also may be used but will need additional tubing
- Elastic band tourniquet
- Alcohol or other preoperative skin preparation
- Clear tape
- Clear adhesive bandage
- Saline flushes
- Clear plastic cup (optional)
Personnel
Scalp vein catheterization is mostly done by a doctor. However, a trained nurse having experience in NICU can also perform scalp vein catheterization.
Preparation
Have another practitioner nearby to restrain the child during the procedure. It may also be helpful to have a parent available to calm and comfort the child. A papoose or swaddling blanket may be helpful to restrain the patient's arms, especially if no assistance is available. The person placing the IV should be at the head of the bed for easier access to the scalp. One drop of oral sucrose may be placed on the infant's tongue or on a pacifier to provide a calming effect.
Technique or Treatment
Veins are visible and can be distended by having the infant cry and using digital pressure at the base of the vein. Catheters should be directed toward the heart. The superficial temporal, frontal, occipital, and pre- and post-auricular veins are suitable for use. It is important to differentiate between arteries and veins, as the scalp may have an impressive arterial network in addition to a selection of veins. It can be difficult to tell the difference before the venipuncture is made. Any inadvertent arterial puncture must be followed by catheter removal and pressure to the site.
To further dilate the scalp veins, place rubber or elastic band above the ears and eyes on the patient's scalp. Make sure the band is not too tight, indicated by red or purplish skin. Areas chosen behind the hairline may allow for a reduction in noticeable scars in the future. A non-tortuous vein must be selected for catheterization. Clean the area with alcohol or preoperative skin preparation. Nearby areas of hair may be shaved to allow for better visualization and proper securing of the catheter. Pull gentle traction on the vein with the non-dominant hand to prevent movement of the vessel and proceed with inserting the needle. An obvious flashback of blood or "pop" when entering the vein may not be present when accessing younger children. Slowly and gently insert the needle parallel to the vessel at 20 to 30 degrees above the skin until you see blood in the chamber. The tourniquet may now be removed. Next, advance the needle slightly to confirm that the needle is in the vein. Allow the infant to calm down before threading the catheter. This mitigates venous spasm. Inject a small amount of saline solution to test the catheter's patency and position. If the saline flushes easily, without evidence of infiltration, then the catheter should be secured in place. Place a small piece of rolled gauze under the catheter hub to prevent pressure on the underlying skin. Apply transparent adhesive dressing to the hub site then adhere several pieces of tape in a crisscross or "H" pattern to secure the device. Also, tape a loop of the loose tubing nearby so that, if pulled on, the loop will give way before the catheter. Some references recommend taping down a half-cut, clear plastic cup over the site for further protection. The base of the cup may be cut to form a hinge for easier access.
Complications
Venous dural sinus air embolism is an inherent risk due to the valveless nature of scalp veins. Injecting air into the scalp vein catheter and leaving it open to air when the infant is in head-up tilt position must be avoided. Preventative measures include supine or Trendelenburg position during daily management of the catheter. An air occlusive dressing should be used once the catheter is removed.[3][4][5]
Puncture site infection may occur if the area is not cleaned properly before needle insertion or if the needle is left in place for an extended period. Research shows that peripheral IVs in children may have a longer duration until bacterial colonization compared to adults. This may be up to 6 days. If IV access is needed for more than one week, a peripherally inserted venous catheter may be considered.
Scalp vein needles provide a lesser risk of infection when compared to plastic catheters. Teflon catheters have the highest rate of phlebitis. Other potential complications include scalp abscess, alopecia, intracranial abscess, thrombophlebitis, and scalp necrotizing fasciitis, all of which are rare.[6][7][8]
Clinical Significance
Scalp veins can be used for peripherally inserted venous catheters without an increase in complications when compared to other insertion sites.
Enhancing Healthcare Team Outcomes
Scalp vein catheterization can be a lifesaving measure in infants who lack peripheral access. The catheterization in most cases is done by the anesthesiologist or the NICU staff. However, the monitoring of these lines is usually done by NICU nurses. However, nurses need to know the potential complications of these lines which can range from an air embolus to dural sinus thrombosis and infection. The site of line insertion has to be regularly cleaned and monitored for infection. Overall, the durability of scalp vein catheterization is much shorter than peripheral lines. In most cases, when peripheral access is obtained, the scalp line is removed.[9]
Nursing, Allied Health, and Interprofessional Team Interventions
Scalp vein catheterization is mostly done by pediatricians or neonatologists. However, nurses trained in NICU are required to know the procedure and its complications. During maintenance of a scalp vein catheter, it is important that the nurses should inspect the site daily and clean it with antiseptics. The child, in whom scalp vein catheterization is done, must be nursed in a Trendelenburg position. It must also be ensured that the hub of the catheter is not kept open and there is no air inside the tubing.